 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
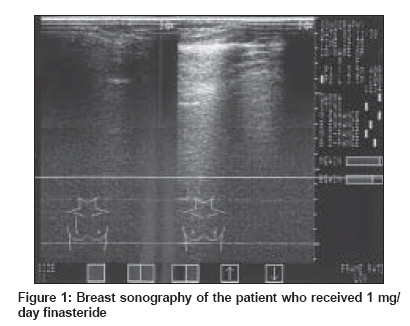
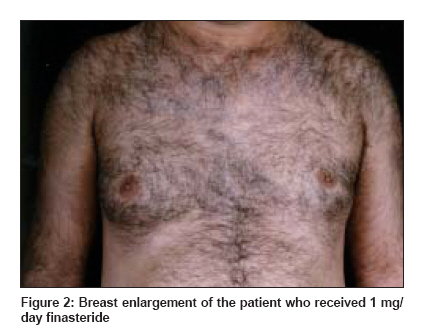
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 309-310 Letter to the Editor Finasteride-induced gynecomastia Mansouri Parvin, Farshi Susan, Safar Farid Department of Dermatology, Imam Hospital, Tehran University of Medical Sciences, Tehran Code Number: dv09094 PMID: 19439893 Sir, Finasteride has successfully been used for treatment of male androgenetic alopecia. [1] Gynecomastia is a rare adverse effect of this drug, which has been reported by some authors, especially at the dose of 5mg/d; [2] few authors have also reported of this complication with 1mg/d finasteride. [1] We also observed the same adverse effect in two patients receiving orally 1mg/d finasteride. Case 1: A 19- year-old man affected by male pattern hair loss (MPHL) received finasteride, 1 mg/d for 8 months. Seven months later, he presented with a painful enlargement of his left breast, with no evident nodules at palpation. On sonography, there was diffuse increase in breast tissue, without any abnormal mass or parenchymal distortion [Figure - 1]. Axillary lymph nodes were normal. Laboratory evaluations including testosterone, free testosterone, luteinizing hormone, dehydroepiandrosterone, and prolactin were within normal range. Dihydrotestosterone level was 135 µg/ 100 mL (normal, 133-441). Follicle-stimulating hormone was 1.1 IU/L (normal, 1.4-10.5). 17-hydroxyprogesterone level was elevated at 3.63 ng/mL (normal, 0.5-2.4). The result of semen analysis was normal. Liver function and thyroid function studies were normal. Any other causes of gynecomastia, including other drug-induced gynecomastia and breast cancer, were ruled out in this patient by endocrine consultation. Treatment was stopped, and 4 months later gynecomastia completely disappeared and laboratory tests returned to normal levels. Two months later, the patient was restarted on the finasteride regimen, 1 mg every alternate day, with no relapse of gynecomastia. Case 2: A 43-year-old man with male pattern hair loss (MPHL) presented with unilateral painful mammary enlargement that had developed 20 days after starting finasteride 1 mg/d. He presented with a gynecomastia of the right breast [Figure - 2], with no evident nodules at palpation. He also noticed a decrease in libido during treatment with finasteride. There was a history of opium use since 20 years, but he had stopped it 6 months before starting the finasteride regimen. Results of hormone studies were normal. He refused to undergo sonography or mammography. Treatment was stopped, and 3 months later the pain decreased, but after 7 months he still had the right breast enlargement. Reduction in serum dihydrotestosterone is a theoretical cause of gynecomastia induced by finasteride. [3] Ferrando et al ., reported four cases of gynecomastia induced by 1 mg/d finasteride. All cases had unilateral gynecomastia and the symptoms disappeared after discontinuation of therapy. [1] Some authors have reported the occurrence of gynecomastia with the use of finasteride for benign prostatic hypertrophy. [2],[4],[5] A similar case of unilateral painful gynecomastia by using 1 mg/day finasteride has been reported by Wade and Sinclair. [3] Our both patients also presented with a unilateral painful gynecomastia, which showed complete resolution in one and partial resolution in the other after cessation of therapy, but Miller et al ., reported recurrent gynecomastia, with finasteride in treating benign prostatic hyperplasia. [5] Continued surveillance and close follow-up of cases on long-term treatments with finasteride are needed for better knowledge of real incidence of gynecomastia. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09094f2.jpg] [dv09094f1.jpg] |
| |||||||||

{kind=link}
{kind=link}