 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
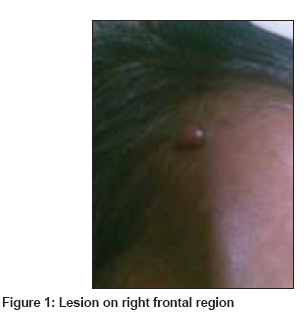
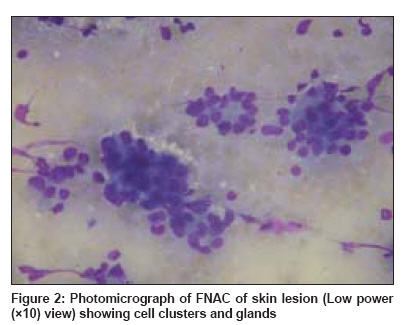
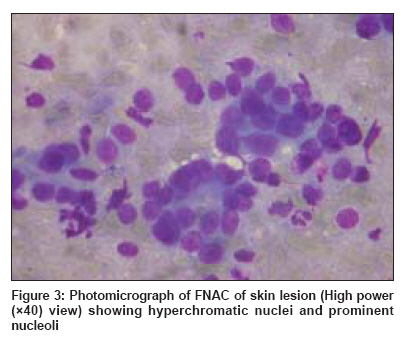
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 311-312 Letter to the Editor Cutaneous metastasis in prostatic carcinoma Pal Devender, Talwar Vineet, Doval DC, Jalpota YP, Kumar Neeraj Rajiv Gandhi Cancer Institute and Research Centre, Rohini Sector-5, New Delhi Code Number: dv09095 PMID: 19439894 Sir, Almost all prostate cancers are adenocarcinoma. The age-specific mortality and absolute number of deaths from prostate cancer have been decreasing since 1993. [1] There is an almost 8:1 ratio in the incidence of prostate-specific mortality. The disease locally invades along the nerve sheath and metastasizes through lymphatic chains or blood vessels. [2] Distant metastases are common when lymph nodes are involved. Bone is the most common site of metastases. Here, we are reporting one patient with metastatic prostatic carcinoma who later developed cutaneous metastases during the course of disease. A 50-year-old man presented with protuberant left eye (without any loss in visual acuity) and increased urinary frequency for the last 6 to 7 months. On examination, he had prostatomegaly, the biopsy of which showed adenocarcinoma of prostate with Gleason′s score of 4+3. CT scan of the head revealed infiltrative lesions involving the left sphenoid bone and left orbit. He also had extensive bone and brain metastases on 99m TcDP whole-body bone scan. He was initially treated with bilateral orchiectomy, External Beam Radio Therapy (EBRT) to brain and was given radioactive phosphorous for bone metastases. He partially responded to the treatment and later received hormone therapy on relapse. Because of the recurrent disease, he received EBRT twice again for spinal/epidural disease. Subsequently, he presented with 3 small, fleshy, painless lesions on the right side of the forehead and bilateral parietooccipital region of the scalp, which were slowly increasing in size over the last 2 to 3 months. On examination, they were 1 x 0.8cm, 0.7 x 0.7cm and 0.5 x 0.5cm, non-tender and firm nodular lesions [Figure - 1]. FNAC and, subsequently, biopsy of the skin lesions revealed malignant cells, with some of them forming glands with hyperchromatic nuclei and prominent nucleoli suggestive of cutaneous metastases of adenocarcinoma of the prostate [Figure - 2] and [Figure - 3]. They were found to be positive for PSA by immunohistochemical staining, thus confirming the prostatic origin of the skin lesions. Between 2% and 9% of visceral malignancies are responsible for cutaneous metastases. [3],[4] They usually occur in the advanced stage of malignancy and are associated with poor prognosis. Although carcinoma of the prostate is common, it is responsible for less than 1% of the skin metastases. [5] Also, skin metastases are a rare manifestation of prostatic adenocarcinoma. Skin metastases from prostate cancer are an ominous finding and most patients die within 6 months. The skin lesions are usually asymptomatic and lower abdomen, genitalia and thighs are most often involved. [6] The head region can also be involved, although rarely seen, as in our case. The lesions are usually papular and they rarely ulcerate. They may have zosteriform distribution or mimic pyoderma. [7] Occasionally, they appear as sclerodermoid lesion. [8] The mechanism of skin involvement is not well understood [2] but suggested routes include embolization of vessels, dissemination via lymphatics [9] and spread through perineural lymphatics. In most cases, where skin metastases have occurred, the primary cancer is widespread and may be advanced. Thus, the treatment is palliative care at this stage which includes keeping the lesion dry and clean. Debridement is an option for bleeding or crusting lesions. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09095f1.jpg] [dv09095f2.jpg] [dv09095f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}