 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
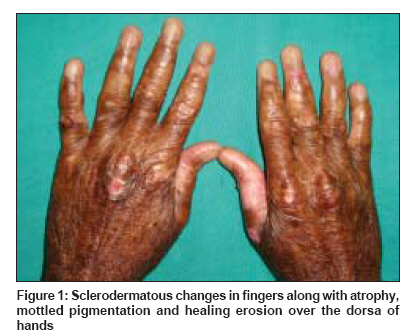
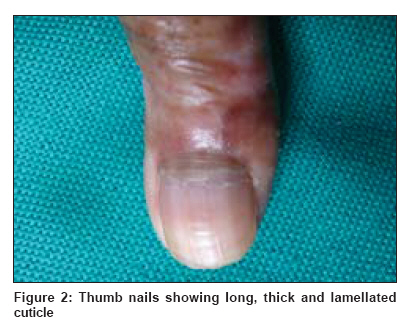
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 314-315 Letter to the Editor Long cuticle of the nail in Kindler's syndrome: Is it more than an incidental finding? Nath AmiyaKumar, Chougule Abhijit, Thappa DevinderMohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006 Code Number: dv09097 PMID: 19439896 Sir, Kindler syndrome (KS) is a rare, autosomal recessive genodermatosis characterized by acral blistering and photosensitivity occurring in early infancy and improving with age, and by the development of generalized progressive poikiloderma and marked cutaneous atrophy. [1] Involvement of the cuticle of the nail in KS is very rare. [2] After keratosis follicularis spinulosa decalvans, [3] it is probably the second disorder, which has been associated with long cuticles of the nails. Herewith, we describe a rare case of KS with long, thick, and fragile cuticles in multiple nails. A 31-year-old male patient, born of a non-consanguineous marriage after an uneventful pregnancy, presented to our dermatology outpatient department with recurrent blistering all over the body and photosensitivity since early infancy. He was normal at birth, but started to develop spontaneous or trauma-induced blistering of the skin soon after birth. The blisters used to arise on normal-looking skin, contain clear fluid with occasional secondary infection or hemorrhage, rupture at times producing raw erosions, and subside after about a week. The frequency of blistering was about 3 to 4 times a month, but the severity of blistering reduced with the increasing age. There was significant photosensitivity restricting outdoor activities. The patient also noticed mottled hyperpigmentation of the skin all over the body since childhood (starting at age 5-6 years). He gave a history of irritation in the eye and occasional oral ulcers. There was no history of discoloration of urine, difficulty in micturition, deglutition, or defecation. There was no history of seizures or neurological disorders. No one in the family or among the relatives suffered from similar disease. On examination, physical and mental development was found to be normal. Extensive mottled hypo- and hyperpigmentation, with atrophy of the skin was noticed involving the skin all over the body except the scalp. Atrophy was marked, and was associated with shiny, cigarette paper-like wrinkled skin and scarring in the hands, feet, elbows and knees. Fingers showed sclerodermatous changes (tapering fingers and bound down skin) [Figure - 1]. Palmoplantar keratoderma, contactures with loss of dermatoglyphics were noticed in the palms. A few healing erosions were seen on the dorsa of fingers [Figure - 1], elbows and shins. Facial skin was shiny, stretched and with mild ectropion of the lower lids, giving an owl-like facies. Nails were normal except for the absent nail in the right great toe. Cuticles in most nails were longer, thicker and fragile, giving a ruffled, lamellated appearance to the cuticle [Figure - 2]. Oral mucosal hyperpigmentation was seen in some areas. Eye examination revealed few papillae on the conjunctiva with squamous blepharitis. Hair shaft examination (microscopy) was normal. On investigation, complete hemogram, blood chemistry, liver and renal function tests were normal. HBsAg, HIV and VDRL tests were negative. Ultrasound abdomen was normal except for cystitis. Histopathology of the non-rubbed poikilodermatous skin showed epidermal atrophy, vacuolar degeneration of the basal cell layer, melanin incontinence, mild inflammatory infiltrates in the dermis, fragmentation of dermal collagen and some vascular ectasias. These findings were consistent with the clinical diagnosis of Kindler′s syndrome. The initial feature of Kindler syndrome is trauma-induced blistering in infancy, often resembling dystrophic epidermolysis bullosa or non-Herlitz junctional epidermolysis bullosa. [4] Later in infancy, recessive dystrophic epidermolysis bullosa (RDEB) might be more specifically considered differentially because of the development of esophageal, anal and/or urethral stenosis. [5] In late childhood and adulthood, progressive poikiloderma becomes more prominent, thereby resembling inherited poikilodermatous syndromes. Nail involvement in Kindler′s syndrome is uncommon, and mostly seen as nail dystrophy, [1],[2],[4],[5],[6] thin nail plate [7],[8] with atrophy, [8] onycholysis, [2],[8],[9] subungual hyperkeratosis, [1] thickening and discoloration of the nail plate, [1] nail fragility, [10] onychodystrophy with Beau′s lines and nail ridging, [11] anonychia, [2] and yellow nails. [12] Penagos et al ., [8] reported loss of the angle of the proximal nail fold. Changes in the cuticle of the nails have been rarely described in the literature. Thomson et al ., [7] described attenuated cuticles of the nails in a 37-year-old man with KS. Aboud et al ., [2] reported long and thick cuticles of the nails in all affected members of a consanguineous Saudi-Arabian pedigree with KS. Our patient also had long, thick cuticles in multiple nails, similar to the findings noted by Aboud et al ., [2] However, the increased fragility and lamellated appearance of the long cuticles were unique in our case. The long cuticle of the nail (described as "high cuticle") reported by van Osch et al ., [3] in multiple members in a pedigree with keratosis follicularis spinulosa decalvans had a smooth appearance. The pathogenesis of the long cuticle is not understood. It may be due to atrophy of the "living" layers of the skin in KS, and a relative sparing of the "dead" horny layer, which forms the cuticle of the nail. A point in favor of this argument could be the fact that the long cuticles in our case were seen in the late atrophic/poikilodermatous stage of the disease. To the best of our knowledge, the combination of these cuticular changes has not been described in any other disorder. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09097f2.jpg] [dv09097f1.jpg] |
| |||||||||

{kind=link}
{kind=link}