 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
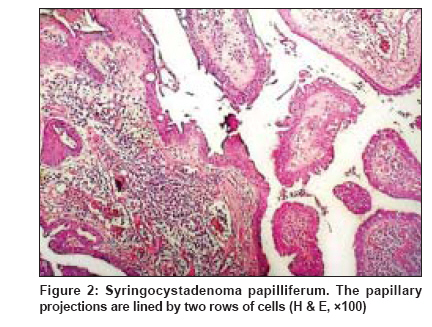
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 318-319 Letter to the Editor Giant linear syringocystadenoma papilliferum on scalp Yaghoobi Reza, Zadeh Sara Hashem, Zadeh Abdoul Hassan Talaie Department of Dermatology, Jondi Shapour University of Medical Sciences, Ahwaz Code Number: dv09100 PMID: 19439899 Sir, A 20-year-old woman, mentally retarded, was brought to the clinic of dermatology with a lesion on left-sided occipital part of the scalp for about 1 year. The lesion was pruritic, bleeding frequently, and increasing in size continuously. An examination of her scalp showed a linear lesion, highly elevated, moist, fetid, vegetated and pinkish, measuring 8 x 3 x 2cm in diameter, on the left side of the occiput with an extension to the nape of her neck [Figure - 1]. A tender lymph node was found in the posterolateral cervical chain. All her routine laboratory tests were within normal limit, with the exception of hypochromic, microcytic anemia. An incisional skin biopsy, with differential diagnoses of organoid nevus, syringocystadenoma papilliferum, leishmaniasis and warty tuberculosis was performed. Histopathological examination revealed a cystic structure in the epidermis containing numerous papillary projections extending into the lumen of cystic structure. These papillary projections were lined by granular epithelium, consisting of two rows of cells. With this finding, the diagnosis of syringocystadenoma papilliferum (SCAP) was made [Figure - 2]. The patient was referred to the general surgeon for total excision of the tumor. Histopathological examination of the total lesion reconfirmed the diagnosis of SCAP, without any malignant transformation and any association with sebaceous nevus. After a 3-month follow-up, no evidence of recurrence was seen. SCAP is a benign adnexal tumor originating from sweat glands. [1] The lesions evolve either de novo or, less frequently, from a sebaceous nevus. [2] SCAP is predominantly a childhood tumor. In about half of those affected, it is present at birth, and in a further 15%-30%, the tumor develops before puberty. [2] SCAP has a varied clinical appearance, usually presents as a hairless, single nodule on the scalp, but a small papular form is also known. [2],[3] In addition to the head and neck, the involvement of other anatomic locations are well documented but uncommon. [2],[4] The lesions of SCAP measure between 1 and 3 cm in diameter [3] and all published cases of nodular SCAP have to date measured < 4 cm in diameter. [4] A vast majority of SCAPs are solitary lesions, and linear arrangement of these lesions is particularly rare. [5] In 2001, Patterson et al ., described that there had been only eight previous cases of linear SCAP. Five of these most recently reported cases occurred on the chest, left arm, neck and right thigh. [5] In contrast to the diverse clinical appearances, the histology of SCAP is uniform and characteristic, offering a reliable tool for the diagnosis. [2] Four characteristic features in the present case encouraged us to report it. These include linear arrangement, giant size, de novo development and no evidence of malignant transformation, despite large dimensions of the tumor. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09100f1.jpg] [dv09100f2.jpg] |
| |||||||||

{kind=link}
{kind=link}