 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
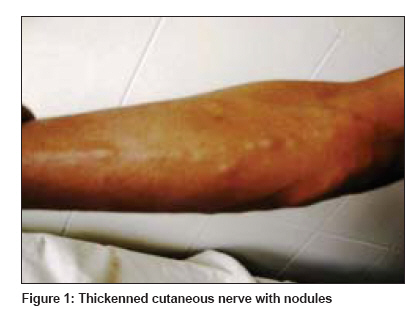
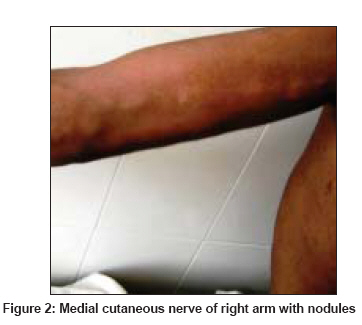
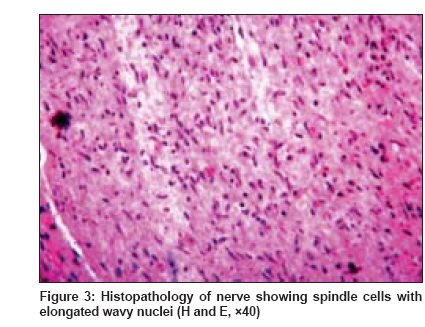
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 319-321 Letter to the Editor Neurofibromatosis presenting as generalized nerve thickening Rao Angoori Gnaneshwar, Danturty Indira, Rekha Teja Narsingh Department of Dermatology, Gandhi Medical College, Secunderabad Code Number: dv09101 PMID: 19439900 Sir, Neurofibromatosis (NF) or von Recklinghausen′s disease is a common autosomal dominant neurocutaneous disorder with a prevalence of 1 in 2500 to 3300 births. [1] Less than 10% occur from spontaneous mutations. [2] It is characterized by tumors arising from peripheral nerves and the central nervous system and hyperpigmented macules (cafι-au-lait macules).The diagnosis is based on the criteria established by the National Institutes of Health (NIH) consensus development conference. [3] Thickening of the peripheral nerves is one of the cardinal features of leprosy. Localized tumors arising from sheaths of peripheral nerves causing nerve thickening can sometimes be seen in neurofibromatosis. A 26-year-old male patient came to the Dermatology outpatient department with multiple nodules over the face, trunk and extremities since childhood, associated with multiple pigmented patches mainly on the trunk. There was no positive family history. Cutaneous examination revealed multiple cafι-au-lait macules and skin colored to reddish brown nodules distributed over the chin, the trunk and the extremities. The nodules were tender and firm in consistency and were found to be mobile. All the peripheral nerve trunks (greater auricular, ulnar, common peroneal and posterior tibial) were uniformly thickened. The medial antebrachial and the lateral antebrachial and posterior antebrachial cutaneous nerves were thickened. There were multiple small nodules along the course of these nerves [Figure - 1] and [Figure - 2]. Axillary freckling was present. There were no hypopigmented patches. There was no neurological deficit. Slit-lamp examination confirmed the presence of Lisch nodules in right eye. CT scan of the brain and ultrasound examination of the abdomen revealed normal results. Audiometry result was unremarkable. Slit skin smears for AFB were negative. Nerve biopsy taken from the radial cutaneous nerve showed well-circumscribed spindle cell lesion composed of irregular cells with elongated wavy nuclei, consistent with features of neurofibroma [Figure - 3]. The results of staining were negative for amyloid deposits. In tropics, leprosy is by far the most common cause of nerve thickening. Universal nerve thickening is rare in neurofibromatosis. Generalized nerve thickening is only sporadically reported in neurofibromatosis. [4],[5],[6] When encountered, such nerve thickening can easily be mistaken for generalized nerve thickening of leprosy. There have been case reports where neurofibromatosis was associated with leprosy. [7],[8] The reported case presented with nerve thickening, cafι-au-lait macules and neurofibromata, which were unmistakable for neurofibromatosis. Leprosy was not considered in the differential diagnosis; however, in patients where there are no cutaneous lesions of neurofibromata the issue cannot be solved without a nerve biopsy. Literature also mentions some other rare causes of universal nerve thickening, such as pachydermoperiostosis, primary amyloidosis, familial hypertrophic interstitial neuritis, Charcot-Marie-Tooth disease, chronic inflammatory demyelinating polyneuropathy, HIV-associated polyneuropathy and cytomegalovirus infection-associated polyneuropathy. Hence, it is pertinent to remember neurofibromatosis as a cause of generalized nerve thickening, lest it creates confusion with leprosy. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09101f3.jpg] [dv09101f1.jpg] [dv09101f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}