 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
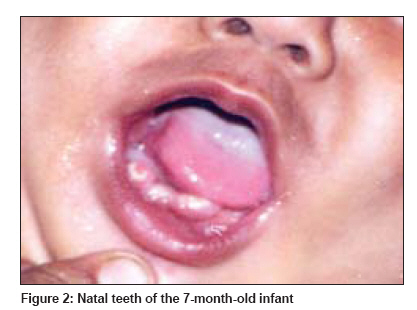
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 321-322 Letter to the Editor Pachyonychia congenita type 2 Das Jayanta Kumar, Sengupta Sujata, Gangopadhyay Asok Department of Dermatology, VIMS, Ramakrishna Mission Seva Pratisthan, 99, Sarat Bose Road, Kolkata - 700 026 Code Number: dv09102 PMID: 19439901 Sir, Pachyonychia congenita (PC) is a rare genodermatosis in which hypertrophy of the nails occurs, in some cases in association with nail bed and hyponychial hyperkeratosis. [1] Autosomal dominant inheritance with incomplete penetrance is the rule, although Haber and Rose described cases with autosomal recessive transmission. [2] The presence of thickened, wedge-shaped nails is the diagnostic clinical feature of PC, but the other clinical characteristics of it usually match with two major patterns. Jadassohn-Lewandowsky syndrome (PC-1) shows focal palmoplantar hyperkeratosis and localized foot blistering, follicular hyperkeratosis and oral leukokeratosis. Jackson-Lawler syndrome (PC-2) shows cutaneous cysts, hair abnormalities and presence of teeth at birth, but less severe nail lesions, and neither oral lesions nor significant keratoderma. [3] About five years ago a 7-month-old male infant, born out of non-consanguineous marriage, presented to us with the complaint of nail defects since birth. On examination, he was found to have thick, brown, wedge-shaped nails with subungual hyperkeratosis, and upward growth of distal nail with angulation of the lateral borders towards the centre. All the proximal nail folds were erythematous and swollen [Figure - 1]. He was also found to have ill-formed lower right incisors and canine teeth. These teeth were present since birth. No other teeth were found to have erupted at the time of examination [Figure - 2]. There was no generalized or focal palmoplantar hyperkeratosis, no hyperhidrosis, no foot blistering, no follicular hyperkeratosis and no cutaneous cysts. Hair and eyes were normal. General examination was normal. There was no family history of similar disorder. The patient was then lost to follow up for a few years. He came recently, after over four years, at the age of five years. There was a gap in the place normally occupied by the left lower incisors and canine as the natal teeth fell prematurely. The other teeth were normal. The examination of the skin and the cutaneous appendages yielded result mostly similar to the examination carried out four years back. But at five years of age the patient had palmoplantar hyperhidrosis, and nail deformity was less severe. The right middle fingernail showed brownish pigmentation, and was thicker than other nails [Figure - 3]. General examination was normal. Complete blood count, routine blood biochemistry, urine analysis and chest X-ray were normal. Culture of the nail scraping taken from the right middle fingernail showed growth of Candida albicans . KOH preparations and fungal culture were uniformly negative from all other toe- and finger-nails. Genetic and molecular biological study could not be done due to lack of infrastructure facility. The patient was treated with fluconazole 100 mg weekly for 12 weeks for the candidal nail infection, and mycological cure was achieved without any corresponding improvement in the appearance of the affected nail. PC is a form of hereditary ectodermal dysplasia with defects in the formation of keratin. A number of purely clinical classifications of this disorder proposed earlier do not correlate satisfactorily with the observed phenotypic expression of all cases. The simple classification of PC into two major patterns, Jadassohn-Lewandowsky syndrome (PC-1) and Jackson-Lawler syndrome (PC-2), is borne out genetically. [4] These two variants of PC arise due to mutations of the genes encoding keratin 6a and 16 in PC-1 (MIM #167200), and 6b and 17 in PC-2 (MIM #167210). [5] There is wide variation in the phenotypic expression, and one study finds the frequency of rarer features such as angular stomatitis and natal or neonatal teeth to be 10% and 16% respectively. [1] Some patients develop chronic oral candidosis. The keratosis is usually benign and requires no treatment except emollients, and acitretin is helpful but not curative; retinoids given for a prolonged period produce some flattening of the nails too. [5] The thickened nails can sometimes be treated surgically. [3] Clinically this case was PC-2. In the differential diagnosis of this case, congenital onychogryphosis was considered. Onychogryphosis does not show dental anomaly, affects predominantly the thumb and large toenails that curve downward at the free margin; but it lacks the subungual hyperkeratosis so characteristic of PC. As no other family members of this case are affected, without genetic study the mode of inheritance remains doubtful. Spontaneous mutations may account for it. There are many reports of PC cases of Indian origin in the literature but none of the cases showed the characteristic dental anomaly of PC-2. Given the low incidence of natal or neonatal teeth (16%), this is understandable. Candidal nail infection was another interesting finding. This led us to consider chronic mucocutaneous candidiasis as a possibility. But in our case the patient did not have any other sign or symptoms of chronic mucocutaneous Candidiasis: he did not have perleche, oral mucosal involvement, or skin involvement similar to chronic mucocutaneous candidiasis. This patient did not have history of other stubborn/recurrent infections. The patient had paronychial inflammation, which is known with pachyonychia congenita too. KOH preparations were uniformly negative from all toe- and finger-nails, and in fungal culture, only the right middle fingernail scrapping showed growth of candidal colonies. In our case we have been able to see the patient after four years, and that enabled us to note the evolution of the lesions with time. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09102f3.jpg] [dv09102f2.jpg] [dv09102f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}