
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 3, 2009, pp. 323-326
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 323-326
Resident's Page
Scoring systems in acne vulgaris
Adityan Balaji, Kumari Rashmi, Thappa Devinder Mohan
Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006
Correspondence Address: Dr. Devinder Mohan Thappa, Department of Dermatology and STD, JIPMER, Pondicherry - 605 006
dmthappa@gmail.com
Code Number: dv09103
PMID: 19439902
DOI: 10.4103/0378-6323.51258
Introduction
Acne vulgaris remains one of the most common diseases afflicting humanity and it is the skin disease most commonly treated by physicians. [1] It is a disease of the pilosebaceous units, clinically characterized by seborrhea, comedones, papules, pustules, nodules and, in some cases, scarring. [2] Although easy to diagnose, the polymorphic nature of acne vulgaris and its varied extent of involvement do not permit simple evaluation of its severity. Because the acne lesions may vary in number during the natural course of the disease, various measurements have been developed, based on clinical examination and photographic documentation, to assess the clinical severity of acne vulgaris. [3] Moreover, if the acne treatment regimens produced an all-or-none response, then acne measurements would be unnecessary. [3]
Grading versus lesion counting
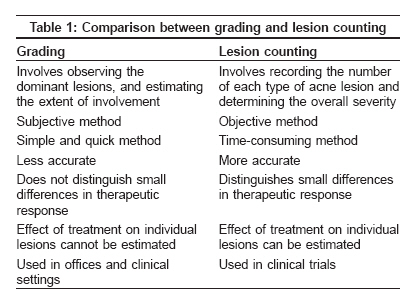
Methods of measuring the severity of acne vulgaris include simple grading based on clinical examination, lesion counting, and those that require complicated instruments such as photography, fluorescent photography, polarized light photography, video microscopy and measurement of sebum production. The two commonly used measures are grading and lesion counting [Table - 1].
Grading is a subjective method, which involves determining the severity of acne, based on observing the dominant lesions, evaluating the presence or absence of inflammation and estimating the extent of involvement. [3] Lesion counting involves recording the number of each type of acne lesion and determining the overall severity.
Photography has also been used as a method of measuring acne severity. Drawbacks of this approach include the following:
- Does not allow palpation to ascertain the depth of involvement. [3]
- Small lesions are often not visualized. [3]
- Maintaining constant lighting, distance between the patient and camera and developing procedure is difficult. [4]
Fluorescence and polarized light photography have some advantages over normal color photography in estimating the number of comedones and emphasizing erythema. However, the disadvantages include problems such as excessive time involvement and the need for more complicated equipment.
Individual methods
Although acne vulgaris has plagued humankind since antiquity, the need for grading acne vulgaris was felt when the therapies available for treating acne increased in the 1950s. Probably, the first person to use a scoring system for acne vulgaris was Carmen Thomas of Philadelphia. She used lesion counting in her office notes, starting in the 1930s. [5] Several systems for grading the severity of acne currently exist.
In 1956, Pillsbury, Shelley and Kligman published the earliest known grading system. [3] The grading includes the following:
- Grade 1: Comedones and occasional small cysts confined to the face.
- Grade 2: Comedones with occasional pustules and small cysts confined to the face.
- Grade 3: Many comedones and small and large inflammatory papules and pustules, more extensive but confined to the face.
- Grade 4: Many comedones and deep lesions tending to coalesce and canalize, and involving the face and the upper aspects of the trunk.
In 1958, James and Tisserand in their review of acne therapy, provided an alternative grading scheme [3]
- Grade 1: Simple non-inflammatory acne - comedones and a few papules.
- Grade 2: Comedones, papules and a few pustules.
- Grade 3: Larger inflammatory papules, pustules and a few cysts; a more severe form involving the face, neck and upper portions of the trunk.
- Grade 4: More severe, with cysts becoming confluent.
The response to acne therapy could never be precisely assessed by grades of 1 to 4 and such classification systems are overly simple. [6] In 1966, Witkowski and Simons [7] initiated lesion counts for assessing the severity of acne vulgaris. Lesions were counted on one side of the face as a time-saving measure, after it was established that the number of lesions of the left side was nearly equal to those on the right.
In 1977, Michaelson, Juhlin and Vahlquist [8] counted the number of lesions on the face, chest and back. They gave a different score to each lesion type. Comedones were valued at 0.5; papules, at 1.0; pustules, at 2.0; infiltrates, at 3.0; and cysts, at 4.0. By multiplying the number of each type of lesion by its severity index and adding each product, these authors obtained a total score that represented the severity of the disease for each visit. This grading system has been criticized on the grounds that scores ascribed to lesions are non-parametric, whereas absolute counts are a parametric data and it is probably wrong to mix these two types of data.
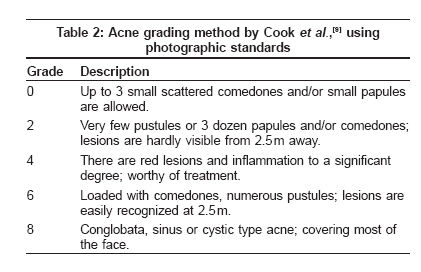
In 1979, Cook, Centner and Michaels [9] evaluated the overall severity of acne on a 0-8 scale anchored to photographic standards that illustrate grades 0, 2, 4, 6 and 8 [Table - 2]. In addition to the photographic standards, a nine-point scale for comedones, papules and macules over the face was used in conjunction for more sensitivity.
In 1984, Burke, Cunliffe and Gibson [10] presented the Leeds technique. They described two scoring systems. The first is an overall assessment of acne severity for use in routine clinic and the second, a counting system for detailed work in therapeutic trials. A scale of 0 (no acne) to 10 (the most severe) was used for grading. The groups 0 to 2 were divided into subgroups, by 0.25 divisions. Grades 0.25 to 1.5 represented patients with physiological acne or "acne minor" and those with grades of 1.5 or more have clinical acne or "acne major."
In 1996, Lucky et al ., [11] assessed the reliability of acne lesion counting. Acne counts were recorded on a template divided into five facial segments: Right and left sides of the forehead, right and left cheeks and chin. The nose and the area around it were excluded. Counts of each lesion type were recorded within each segment of the template. Total lesion count, along with total inflammatory lesions and comedonal counts, were then calculated. They concluded that reliability of acne lesion counting was excellent when performed by the same trained rater over time.
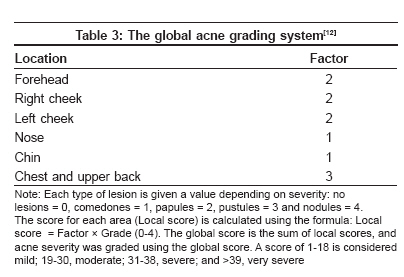
In 1997, Doshi, Zaheer and Stiller [12] devised a global acne grading system (GAGS). This system divides the face, chest and back into six areas (forehead, each cheek, nose, chin and chest and back) and assigns a factor to each area on the basis of size [Table - 3].
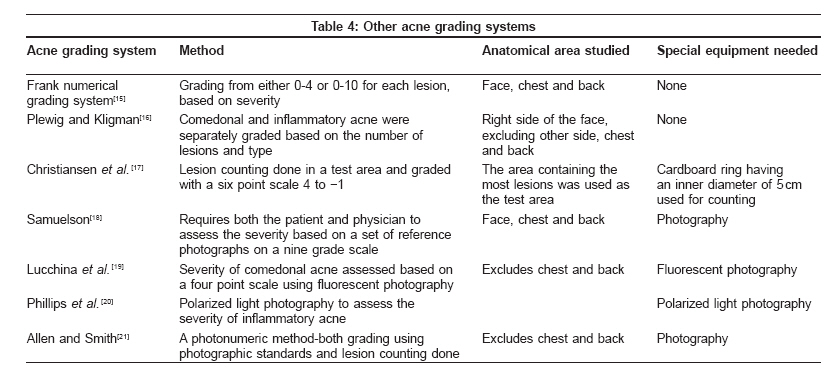
In 2008, Hayashi et al. , [13] used standard photographs and lesion counting to classify acne into four groups. They classified acne based on the number of inflammatory eruptions on half of the face as 0-5, "mild"; 6-20, "moderate"; 21-50, "severe"; and more than 50, "very severe." Other grading systems used for grading acne vulgaris are summarized in the [Table - 4].
Acne vulgaris was graded by Indian authors, [14] using a simple grading system, which classifies acne vulgaris into four grades as follows.
- Grade 1: Comedones, occasional papules.
- Grade 2: Papules, comedones, few pustules.
- Grade 3: Predominant pustules, nodules, abscesses.
- Grade 4: Mainly cysts, abscesses, widespread scarring.
Conclusion Assessment of the severity of acne vulgaris continues to be a challenge for dermatologists. No grading system has been accepted universally. An ideal grading system would
- Be accurate and reproducible.
- Capable of documentation for future verification.
- Be simple to use by the clinician over serial office visits.
- Be less time consuming.
- Be less expensive and simple.
- Reflect subjective criteria, i.e., psychosocial factors.[21]
References
| 1. | Gelmetti CC, Krowchuk DP, Lucky AW. Acne. In: Schachner LA, Katz SI, editors. Pediatric Dermatology, 3 rd ed., Philadelphia: Mosby; 2003. p. 589-609. Back to cited text no. 1 |
| 2. | Simpson NB, Cunliffe WJ. Disorders of sebaceous glands. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology, 7 th ed., Oxford: Blackwell publishing; 2004. p. 43.1 - 43.75. Back to cited text no. 2 |
| 3. | Witkowski JA, Parish LC. The assessment of acne: An evaluation of grading and lesion counting in the measurement of acne. Clin Dermatol 2004;22:394-7. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Burke BM, Cunliffe WJ. The assessment of acne vulgaris: The Leeds technique. Br J Dermatol 1984;111:83-92. Back to cited text no. 4 |
| 5. | Witkowski JA, Parish LC. From the ghosts of the past: Acne lesion counting. J Am Acad Dermatol 1999;40:131. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Shalita AR, Leyden JJ Jr, Kligman AM. Reliability of acne lesion counting. J Am Acad Dermatol 1997;37:672. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Witkowski JA, Simons HM. Objective evaluation of demethylchortetracycline hydrochloride in the treatment of acne. JAMA 1966;196:397-400. Back to cited text no. 7 [PUBMED] |
| 8. | Michaelsson G, Juhlin L, Vahlquist A. Oral zinc sulphate therapy for acne vulgaris. Acta Derm Venereol 1977;57:372. Back to cited text no. 8 |
| 9. | Cook CH, Centner RL, Michaels SE. An acne grading method using photographic standards. Arch Dermatol 1979;115:571-5. Back to cited text no. 9 [PUBMED] [FULLTEXT] |
| 10. | Burke BM, Cunliffe WJ. The assessment of acne vulgaris: The Leeds technique. Br J Dermatol 1984;111:83-92. Back to cited text no. 10 |
| 11. | Lucky AW, Barber BL, Girman CJ, Williams J, Ratterman J, Waldstreicher J. A multirater validation study to assess the reliability of acne lesion counting. J Am Acad Dermatol 1996;35:559-65. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading systems and proposal of a novel system. Int J Dermatol 1997;36:416-8. Back to cited text no. 12 [PUBMED] |
| 13. | Hayashi N, Akamatsu H, Kawashima M. Acne Study Group. Establishment of grading criteria for acne severity. J Dermatol 2008;35:255-60. Back to cited text no. 13 |
| 14. | Tutakne MA, Chari KVR. Acne, rosacea and perioral dermatitis. In: Valia RG, Valia AR, editors. IADVL Textbook and atlas of dermatology, 2 nd ed., Mumbai: Bhalani publishing House; 2003. p. 689-710. Back to cited text no. 14 |
| 15. | Frank SB. Acne vulgaris. Springfield, IL: Thomas, 1971. p. 12-3. Back to cited text no. 15 |
| 16. | Plewig G, Kligman A. Acne: morphogenesis and treatment. New York: Springer-Verlag; 1975. p. 162-3. Back to cited text no. 16 |
| 17. | Christiansen J, Holm P, Reymann F. Treatment of acne vulgaris with the retinoic acid derivative Ro 11-1430. A controlled clinical trial against retinoic acid. Dermatologica 1976;153:172-6. Back to cited text no. 17 |
| 18. | Samuelson JS. An accurate photographic method for grading acne: Initial use in a double-blind clinical comparison of minocycline and tetracycline. J Am Acad Dermatol 1985;12:461-7. Back to cited text no. 18 |
| 19. | Lucchina LC, Kollias N, Phillips SB. Quantitative evaluation of noninflammatory acne with fluorescence photography. J Invest Dermatol 1994;102:560. Back to cited text no. 19 |
| 20. | Phillips SB, Kollias N, Gillies R, Muccini JA, Drake LA. Polarized light photography enhances visualization of inflammatory lesions of acne vulgaris. J Am Acad Dermatol 1997;37:948-52. Back to cited text no. 20 [PUBMED] [FULLTEXT] |
| 21. | Allen BS, Smith JG Jr. Various parameters for grading acne vulgaris. Arch Dermatol 1982;118:23-5. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09103t3.jpg]
[dv09103t4.jpg]
[dv09103t2.jpg]
[dv09103t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}