 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
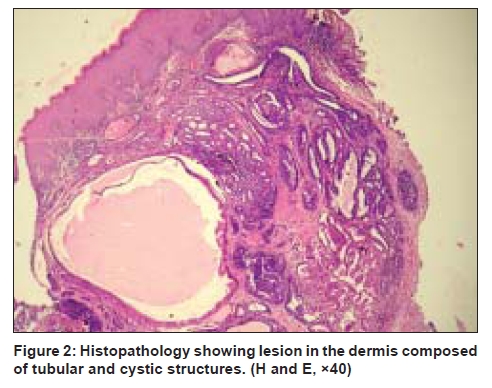
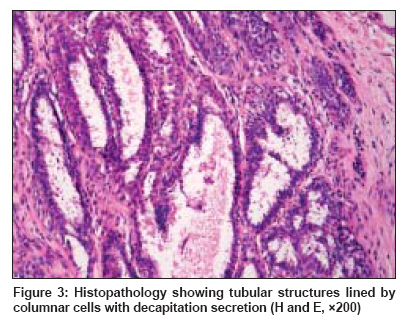
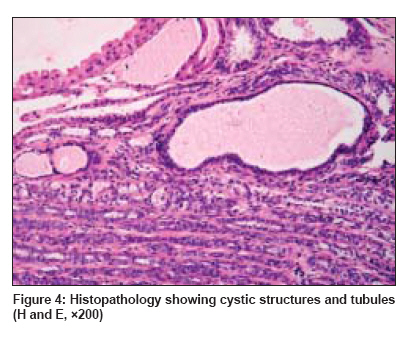
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 327-328 Quiz Solitary nodule over the labia majora Veeranna S, Vijaya Department of Skin and STD, J.S.S Hospital, Mysore, Karnataka Code Number: dv09104 PMID: 19439903 A 35-year-old woman presented with an asymptomatic solitary lesion on the labia majora for the past 6 months. The lesion started as a small swelling and gradually increased in size. There was no history of pain, itching, bleeding or discharge. On examination, there was a solitary nodule measuring 1 x 1 cm situated on the inner aspect of the right labia majora [Figure - 1]. The surface was eroded. There was no tenderness or induration. There was no regional lymphadenopathy. Hemogram and urin-analysis was normal. Blood Venereal Disease Research Laboratory (VDRL) and HIV test results were negative. Excision biopsy was done. Histopathology findings are shown in [Figure - 2],[Figure - 3],[Figure - 4]. What is your diagnosis ? Diagnosis: Hidradenoma papilliferum Discussion Hidradenoma papilliferum is a rare, benign, cystic, papillary apocrine gland tumor that occurs almost exclusively in the skin of the anogenital region in women. [1] It occurs between the ages of 25 and 40 years. [2] It usually presents as an asymptomatic nodule measuring 1 to 40 mm in size. The most common site is the labia majora, but it may occur elsewhere on the vulva or perianal area. Other ectopic sites include eyebrow, eyelid, nose, chest and external auditory canal. [3] Ectopic hidradenoma papilliferum occurs more frequently in the head and neck region. It is rarely associated with Paget′s disease and invasive squamous cell carcinoma. [4] The tumor represents an adenoma with apocrine differentiation. Hidradenoma papilliferum can also originate from recently described anogenital mammary-like glands. [5] Located in the dermis, it is well circumscribed and surrounded by a fibrous capsule. The tumor is usually partly cystic and comprises of both papillary and glandular areas. The lumina are lined by single or double layer of cells consisting of a luminal layer of secretory cells, which show active decapitation secretion, and an outer layer of small cuboidal cells. [6] The tumor is usually mistaken for a cyst, polyp or an angioma. The histopathological differential diagnosis includes tubular apocrine adenoma, syringocystadenoma papilliferum, apocrine hydrocystoma and apocrine fibroadenoma. [6] Simple excision is curative. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09104f4.jpg] [dv09104f3.jpg] [dv09104f1.jpg] [dv09104f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}