 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
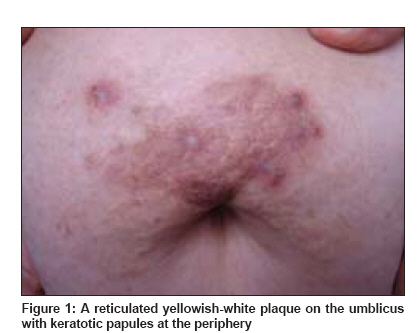
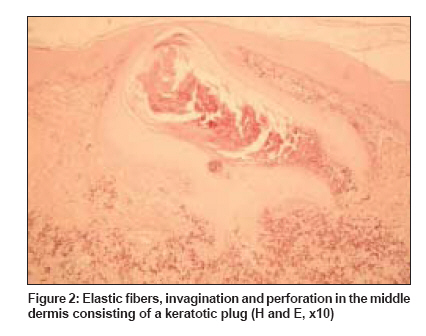
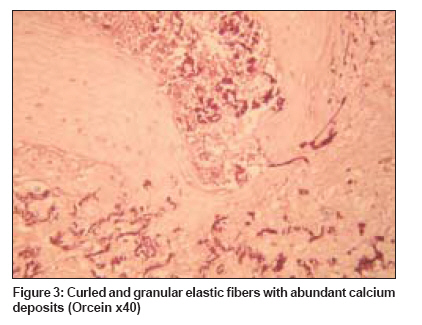
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 329 Net Case Periumbilical perforating pseudoxanthoma elasticum Kocaturk Emek, Kavala Mukaddes, Zindanci Ilkin, Koc Melek Goztepe Training and Research Hospital, Department of Dermatology, Istanbul Code Number: dv09106 PMID: 19439905 Abstract A 58-year-old, gravida 6, obese woman presented with a pruritic yellowish plaque around the umbilicus, which first appeared about 3 years ago. She also had flat yellow papules on the axilla and neck. After a burn from a heating device, a few perforating papules and a violaceous hue occurred on the plaque. Histological examination revealed pathological elastic fibers with a keratotic plug and perforation in the deep dermis, which was consistent with perforating pseudoxanthoma elasticum. This case indicates that perforating pseudoxanthoma elasticum, a variant of hereditary pseudoxanthoma elasticum may perforate due to mechanical factors.Keywords: Localized pseudoxanthoma elasticum, Perforating calcific elastosis, Periumbilical perforating pseudoxhantoma elasticum Introduction Periumbilical perforating pseudoxanthoma elasticum (PPPXE) usually presents with well-demarcated, hyperpigmented, periumbilical plaques with keratotic papules at the periphery. The histopathology reveals morphologically altered and calcified elastic fibers throughout the dermis that are extruded to the skin by transepidermal elimination. [1] The case reported indicates that perforating pseudoxanthoma elasticum, a variant of hereditary pseudoxanthoma elasticum may perforate due to mechanical factors.Case Report A 58-year-old, gravida 6, obese woman presented with a pruritic plaque on the abdomen. She recognized yellowish flat papules around the umbilicus about 3 years ago. After a burn resulting from a direct contact with a heating device, a few keratotic papules and a violaceous hue occurred on the plaque. Her medical history was notable for hypertension, gastritis, osteoporosis, and hepatitis C infection. Hepatitis C was diagnosed four years ago and was treated with interferon a-2b for nine months. Her family history was unremarkable. On examination, a reticulated plaque with keratotic papules on the umbilicus and flat yellowish papules on the neck and axillary folds were noted [Figure - 1]. Results of routine laboratory tests were normal, except for those of SGOT 100 U/L (0-31), SGPT 50 U/L (0-31), phosphate 4.6 mg/dL (2.5-4.2) and anti-HCV positivity. Abdominal ultrasonography, echocardiography, and fundus angiography were found to be normal. Two punch biopsy specimens were taken; one from the yellowish flat papules and one from the keratotic papules. The former showed curled and granular elastic fibers consistent with pseudoxanthoma elasticum and the latter showed pathological elastic fibers with a keratotic plug and perforation in the deep dermis that was consistent with perforating pseudoxanthoma elasticum. Staining of the two specimens with orcein revealed curled and granular elastic fibers and staining with von Kossa revealed the rich calcium component of the fibers [Figure - 2] and [Figure - 3]. A trial of therapy with topical steroids and topical retinoic acids yielded no benefits.Discussion Formerly known as PXE coexisting with elastosis perforans serpiginosa (EPS), PPPXE is redescribed by Lund and Gilbert as a distinct entity. They analyzed seven cases and found a coexistence of PXE and EPS in only one case. While in EPS the abnormal elastic fibers are located superficially and are unmineralized, in PPPXE elastic fibers are fragmented, clumped and calcified, which are located in the mid and lower dermis. [2] The term PPPXE was first proposed by Hicks et al. , in 1979. [3] Later, Neldner and Martinez- Hernandez proposed the term "localized acquired cutaneous pseudoxanthoma elasticum," as they believed the process was "acquired" and was lacking "systemic involvement". [4] The classification of PPPXE is still controversial. In some cases, it occurs as a localized lesion without systemic involvement of hereditary PXE; typical patient is a multiparous, obese, middle aged, black woman with multiple abdominal surgery or trauma. That is why some authors suggest that it is an acquired localized form seperated from hereditary PXE. [3],[5],[6] Other cases are reported to have angioid streaks and flexural lesions that are suggestive of hereditary systemic PXE. [2],[7],[8] Several patients had accompanying hypertension and diabetes; [2],[3],[4],[6],[7],[9],[10],[11],[12] it is well known that cardiovascular involvement of PXE may lead to renovascular hypertension, and diabetes may also be associated with PXE. [9] These findings brought the idea of an opposing theory that suggests PPPXE as a limited cutaneous manifestation of hereditary PXE in which transepidermal elimination occurs secondarily. [9] Besides these, according to the major and minor criteria for the definition of PXE defined in a consensus conference in 1994, the term "perforating calcific elastosis (PCE) was suggested for cases presenting in obese and multiparous women to emphasize the lack of systemic symptoms. [13] Finally, Sapadin et al. , considered PPPXE as a nosologic bridge between the pure acquired form and the pure inherited form. [1] We found 23 cases in the literature. Of these, 12 were African-American (54%), 17 were multiparous (72%), 14 had hypertension (63%) and 4 had chronic renal failure (18%). [1],[5],[6],[9],[12] Moreover, with regard to the available literature, 4 of them had flexural lesions (18%), whereas 5 had angioid streaks (only 2 of them confirmed with fundus angiography) (22%). [2],[7],[8] The repeated trauma of pregnancy, obesity and/or abdominal surgery may result in elastic fiber degeneration in these patients. [6] The presence of PPPXE in patients with chronic renal failure who had an abnormal phosphate- calcium metabolism, also suggested that as in tumoral calcinosis the calcium deposition in the skin may lead to transepidermal elimination. [1],[6],[7] Our patient had hypertension and flexural lesions suggesting a systemic involvement of PXE. We believe that perforation of these lesions occurred secondarily. She had an unexplained hyperphosphatemia-without chronic renal failure parathyroid gland disease-and had a history of burn trauma on the site of the lesions. One of these factors or all of these together might have led to transepidermal elimination. In conclusion, we believe that PPPXE is a variant of hereditary PXE. Remembering that mild forms of hereditary PXE exist, cases that were referred to as acquired localized form may be mild variants of hereditary PXE. If perforation occurs in a PXE plaque, considering the nature of perforating disorders, in the absence of a mechanical cause such as multiparity, multiple surgery or trauma, one must search for possible metabolic abnormalities such as chronic renal failure or parathyroid diseases. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09106f2.jpg] [dv09106f3.jpg] [dv09106f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}