 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
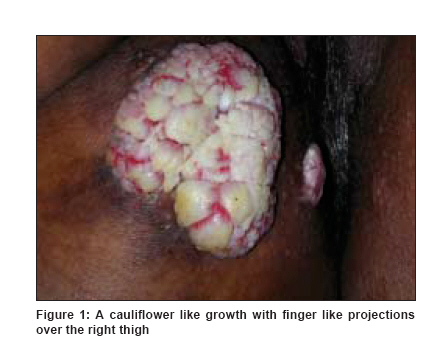
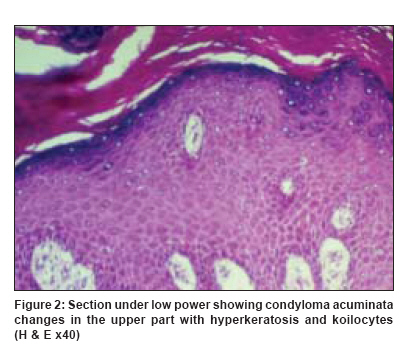
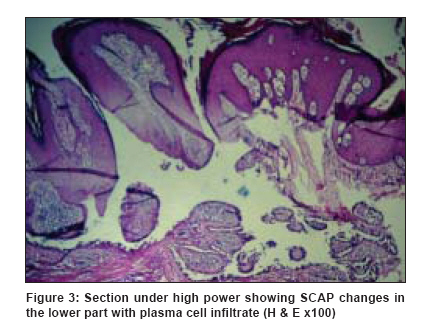
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 330 Net letter Giant condyloma acuminata with syringocystadenoma papilliferum Sardesai Vidyadhar R, Agarwal Vaishali M, Manwatkar Pradnya P, Gharpuray Mohan B Bharati Vidyapeeth University Medical College, Pune - 43 Code Number: dv09108 PMID: 19439910 Sir, Syringocystadenoma papilliferum (SCAP) is classified as a benign tumor [1] of apocrine differentiation. It either develops independently or is commonly seen in association with nevus sebaceous. [2] Giant condyloma acuminata of Buschke and Lowenstein is a slow growing, locally destructive plaque of unknown origin. It was first described by Buschke and Lowenstein in 1925. It is commonly seen over the penis but is also seen in the anogenital region. It has been associated with human papillomavirus types 6 and 11 and less commonly with HPV types 16 and 18. [3] The association of SCAP and giant condyloma acuminata is rare. The occurrence of condyloma acuminata with SCAP may be related to the environment at the surface of SCAP. [4] We report this case to highlight the rare association of two conditions of different etiologies. Two cases have been reported so far in the literature. A 30-year-old married woman presented with two asymptomatic skin lesions on medial aspect of the right thigh for last five years. She had similar skin lesion on the same site 12 years back, for which chemical cauterization was done repeatedly, with no response. An excision biopsy was then done. There was a recurrence of lesion on the excision site after six months. The same lesion had gradually increased to attain the present size. Family and personal history were not contributory. Dermatological examination revealed two skin lesions on the medial aspect of the right thigh [Figure - 1]. The larger one was 6 x 7cm in size and smaller one was 1 x 3cm in size. Both were firm in consistency, non-tender, mobile on the underlying structure, cauliflower-like mass with finger-like projections on the surface. Results of routine blood investigations and serology for HIV/VDRL/HBsAg were negative. Histopathological examination of skin biopsy showed changes in condyloma acuminata in the upper part and SCAP in the lower part of the section [Figure - 2] and [Figure - 3]. Changes of condyloma acuminata were seen as hyperkeratosis, hypergranulosis, koilocytosis in stratum spinosum, and irregular acanthosis with rete ridges converging to the center. Mild mononuclear infiltrate was seen in the dermis. In the lower part of the section, there were changes of SCAP, showing cystic invaginations with numerous papillary projections. Each papilla was lined by two rows of glandular epithelium. The luminal layer was of columnar epithelium covered with eosinophilic active decapitation secretion. The outer layer consisted of cuboidal epithelium. Stroma showed infiltration with plasma cells. DNA probes (AffiProbe test kit) for HPV was negative. SCAP is an uncommon, benign tumor of disputed histogenesis, with a recent theory suggestive of its apoeccrine origin. Typically, it presents as a hairless plaque on scalp associated with nevus sebaceous. At puberty, it becomes larger, nodular and often verrucous. The uncommon sites of presentation are chest, upper arms, male breast, eyelids, scrotum, and thigh. It could be associated with condyloma acuminata. [4] Rarely, it can also be associated with verrucous tumor. [5] Although, the concurrent occurrence of SCAP and giant condyloma acuminata in this patient may be coincidental, it would seem more likely that the transition zone between the epidermis and epithelium of SCAP provided a site more conducive for infection by HPV 6 and HPV 11 than normal dry, keratinised epidermis. Though confirmation of condyloma acuminata by DNA probes for HPV in this case was negative, the location of lesion and clinicopathological correlation was convincing for superimposed HPV infection to be considered. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09108f1.jpg] [dv09108f3.jpg] [dv09108f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}