 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
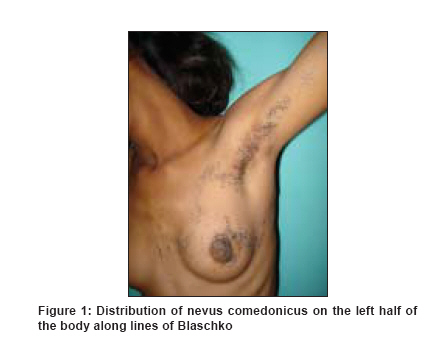
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 330 Net letter Nevus comedonicus along Blaschko's lines Bhagwat P.V., Tophakhane R.S., Rathod R.M., Tonita Noronha M., Naidu Varna Departments of Skin and STD, Karnataka Institute of Medical Sciences, Hubli, Karnataka Code Number: dv09109 PMID: 19439909 Sir, Nevus comedonicus is an uncommon skin abnormality first described in 1895 by Kofmann who used the term "comedo-nevus". It comprises of groups of pits filled with black keratinous plugs resembling blackheads, with inflammatory acne lesions developing later. Nevus comedonicus is caused by a defect in the development of the hair follicle. Lesions may develop any time from birth to middle age, but are usually present at birth or develop before the age of 10 years. Men and women are equally affected. There is no racial predilection. We herewith report a case of nevus comedonicus distributed only over the left half of the body along the Blaschko′s lines and not associated with any systemic abnormalities. A 14-year-old girl, born of a third-degree consanguinous marriage, came to us recently, with multiple grouped pits filled with black plugs over left cheek, left side of the trunk and left upper and lower limbs, which were present since birth. She also had a painful swelling in the lesion over abdomen for the past eight days. She had attained menarche three months back. There was no history suggestive of skeletal, ocular or other systemic involvement. There was no history of any skin disease in the past. No one else in her family had similar complaints. Cutaneous examination revealed groups of dilated follicular openings filled with black, hard plugs, distributed over left cheek, left arm and forearm, left side of the chest [Figure - 1], abdomen, left thigh and left leg along Blaschko′s lines. The lesions over the abdomen revealed a nodulocystic swelling associated with purulent discharge [Figure - 2]. The right half of the body and palms and soles over both sides were spared. Routine hematological investigations including complete hemogram, biochemical parameters, liver function tests and renal function tests were within normal limits. Results of urine and stool examinations were normal. Punch biopsy taken from a lesion over the left thigh was subjected to histopathological examination. It revealed deep, wide invagination of acanthotic epidermis, filled with concentric lamellae of keratin. Hair shafts were occasionally seen in the dermis, below the lower part of the invagination. These histopathological features were consistent with the diagnosis of nevus comedonicus. Comedo nevus is a rare nevus. It can present as single or multiple lesions. It may be linear, interrupted, unilateral, bilateral, present in a dermatomal distribution, along the lines of Blaschko, or segmental. Most common sites of distribution are face, neck, trunk and upper arm. Palms, soles and the glans penis are occasionally involved. [1] Clinically, nevus comedonicus is of two types. In the first type, comedones are predominantly seen. In the second type, comedones undergo inflammatory changes, with late sequelae such as scars, keloids, fistulae and formation of follicular cysts. Our case falls into the first group. In a case report by Klein, the patient presented with nevus comedonicus with extensive involvement of trunk and extremities on the left half of the body with palmar and plantar involvement. [2] The lesions were distributed dermatomally. In another case report by Murthy, a-29-year-old patient presented with unilateral nevus comedonicus along the right eighth thoracic dermatome. [3] Beerman and Homan described a woman in whom recurrent infections in the nevus developed at puberty. [4] Our patient had unilateral distribution over the left half of the body along Blaschko′s lines and there was involvement of face. Nevus comedonicus syndrome is the association of nevus comedonicus with abnormalities of the central nervous system, skeletal system, skin and eye. Central nervous system involvement includes epilepsy, electroencephalogram abnormalities and transverse myelitis. Skeletal system abnormalities include scoliosis, hemivertebrae, spina bifida occulta, foot deformities, absence of fingers, syndactyly and supernumerary digits. Cutaneous associations include ichthyosis, trichilemmal cysts, leukoderma, white hairs, Sturge-Weber syndrome and hemangiomas. Ocular abnormalities include congenital cataracts, either unilateral or bilateral. Our patient did not have any systemic abnormalities. Treatment of nevus comedonicus includes surgical excision, which is more effective in the long term than superficial shaving or dermabrasion. Regular use of a comedo extractor may be useful to achieve cosmetic improvement. Both topical retinoic acid (0.025%-0.1%) and 12% ammonium lactate lotion may improve the appearance of lesions and help prevent secondary inflammation. None of these therapies are very satisfactory. One author suggests that since complications are rarely produced other than inflammation and secondary infection, it is probably better to do nothing unless symptoms arise. [5] We are reporting this case because our patient had extensive lesions and the lesions were distributed unilaterally. Our patient had lesions over the face. These features are rarely described in the literature. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09109f1.jpg] [dv09109f2.jpg] |
| |||||||||


{kind=link}
{kind=link}