 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
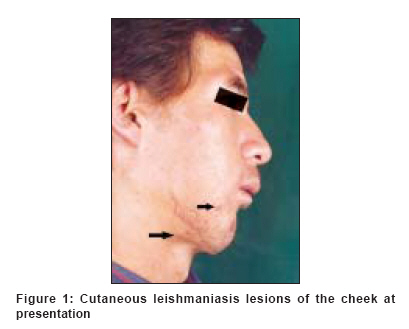
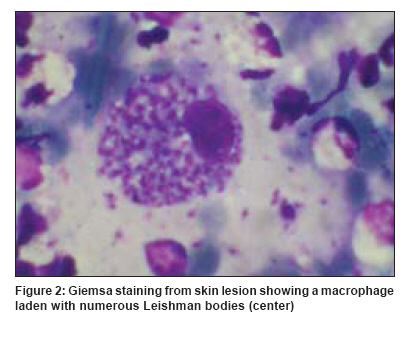
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 3, May-June, 2009, pp. 330 Net letter Facial leishmaniasis mistaken for pimples Motamedi Mohammad Hosein Kalantar, Harandi Parvin Alami, Azizi Taghi Trauma Research Center, Baqiyatallah Medical Sciences University, Attending Faculty, Azad University of Medical Sciences, Tehran Code Number: dv09110 PMID: 19439908 Sir, Leishmaniasis is a parasitic disease caused by the hemoflagellate Leishmania spp . The parasite is transmitted by the bite of an infected female Phlebotomine sandfly. Cutaneous leishmaniasis (CL) occurs throughout Africa, Asia, South America, the Middle East, and the Mediterranean regions. It is a disease with diverse clinical manifestations, which poses a public health problem in endemic countries. [1] According to the geographic region in which different Leishmania species are found and the host response, this disease can affect the skin, viscera, or mucocutaneous areas. Infections with Leishmania are increasing worldwide because of tourism and job-related travel and refugees. [2] In patients with a weak immune response, the reticuloendothelial system is laden with infected macrophages, whereas in subjects with an increased immune response, granulomas form in the lymph nodes, liver, and spleen, with few clinical symptoms. [3],[4] The life cycle of the parasite involves two stages: The amastigote (Leishman-Donovan body) is present in hosts such as humans, dogs, and rodents. The parasite invades and multiplies in macrophages and other reticuloendothelial (RE) cells, which rupture and release the organisms into the bloodstream. When the female sandfly bites an infected host, the amastigotes enter the sandfly and develop into infective promastigotes. The cycle is completed when the sandfly bites another host. A localized lesion may form at the site of the insect bite. In endemic areas, permanent immunity develops to a particular species of Leishmania , with unapparent infection. It is therefore important that clinicians are able to recognize the cutaneous lesions and unusual presentations of CL. [4] Clinicians in rural and remote areas may be the first to confront such patients presenting with cutaneous or mucocutaneous leishmaniasis. Patients presenting with nonhealing papular lesions require smear samples from the depth of the lesions and staining with Giemsa or hematoxylin- eosin and recognition of the parasite or Donovan bodies via light microscopy. Our case was an incidental finding during treatment of a patient suffering from a gunshot wound. The lesion was mistaken for facial pimples because they were numerous and the patient was young. A 19-year-old male war refugee from Afghanistan presented to our clinic with a defect of the right body of the mandible after a gunshot wound in Afghanistan. Clinically, the skin and mucosa of the entrance and exit wounds of the bullet had healed. Several small, painless, papular lesions with indurated, erythematous borders, and central ulcerations were evident on the forehead and cheek [Figure - 1]. The medical history was not significant and the patient was in good health. The patient underwent reconstruction of his bone defect via bone graft. The patient received prophylactic antibiotics (cephalothin, gentamicin, and metronidazole) during the first postoperative week to prevent infection. He was prescribed cephalexin, which he took for the next three weeks. After 2 months, the patient was referred for follow-up. It was noticed that the pustular lesions were still present on the face and had enlarged slightly despite the extensive antibiotic therapy (which often cures ordinary pimples) during this time period. Thus, smears and biopsies were done for the lesions under local anesthesia and submitted for pathologic examination. Light microscopy showed skin with hyperkeratosis, parakeratosis, and acanthosis. The dermis was filled with aggregates of large, pink, histiocytes, and mixed chronic inflammatory cells. The histiocytes contained dot-like organisms typical of cutaneous leishmaniasis [Figure - 2]. Treatment was started with sodium stibogluconate for 3 weeks (intramuscularly 20 mg/kg daily for 21 days). The lesions disappeared and there has been no recurrence 5 years later. Leishmaniasis is an intracellular infection caused by the protozoa Leishmania , transmitted by the sandfly. In the United States, it continues to be the most common deployment-related illness. [5],[6] CL caused by L. tropica is endemic in Pakistan and Afghanistan.[1] Different forms of CL, mucocutaneous (MCL) or visceral leishmaniasis (VL) may develop. CL may heal spontaneously, with scarring or evolve into diffuse CL, with reduced immune response. [1],[2],[3] CL presents with painless nodules with a characteristic erythematous raised border similar to pimples. The lesions heal over months or years when it goes unnoticed, leaving a scar. The causative species of CL determines the clinical features, course, and treatment. Intralesional or systemic antimonials are the gold standard for the treatment. Paromomycin ointments are effective in L. major, L. tropica, L. mexicana, and L. panamensis . In L. braziliensis localized leishmaniasis, both paromomycin and imiquimod may be topically applied. Oral fluconazole and zinc sulfate are useful in L. major . Intramuscular pentamidine is required for L. guyanen CL, for which systemic antimony is not effective. [7],[8] Smears and biopsies should be done for any lesion present for 2 weeks under local anesthesia and submitted for examination to ensure proper diagnosis and treatment by the clinician. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09110f1.jpg] [dv09110f2.jpg] |
| |||||||||

{kind=link}
{kind=link}