 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
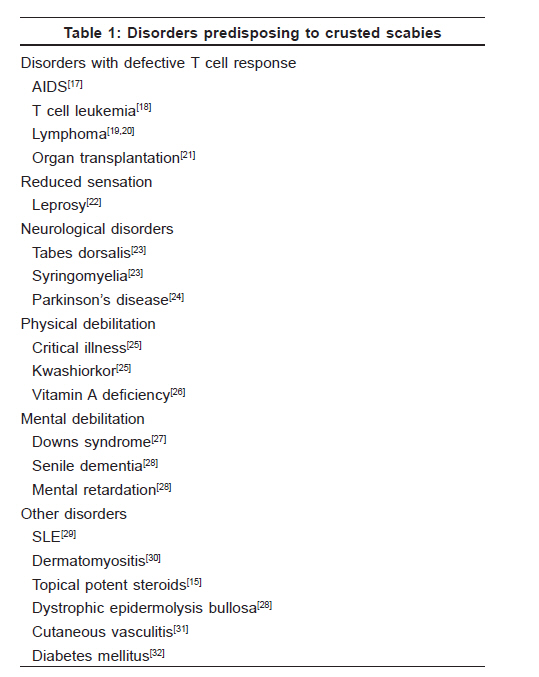
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 340-347 Review Article Crusted scabies Karthikeyan Kaliaperumal Sri Manakula Vinayagar Medical College, Kalitheerthalkuppam, Pondicherry Code Number: dv09141 PMID: 19584457 Abstract Crusted scabies is a rare manifestation of scabies characterized by uncontrolled proliferation of mites in the skin. In immunocompromised patients, this infestation is characterized by crusted lesions. The occurrence of the disease in human immunodeficiency virus-infected patients and the widespread use of immunosuppressive agents has led to a renewed interest in the disease. Early recognition and treatment is necessary to avoid an outbreak of scabies. This review highlights the pathogenesis, predisposing factors, clinical features and treatment of crusted scabies.Keywords: Crusted, Norwegian, Scabies Introduction Crusted scabies was described by Boeck and Danielssen among lepers in Norway in 1848. [1] It was named as "Scabies Norvegi Boeki" by von Hebra in 1862. This severe variant of scabies occurs as widespread hyperkeratotic crusted lesions and hence the name "crusted scabies" is preferred to the eponym of "Norwegian scabies." [2] Crusted scabies is characterized by hyperkeratosis and crusting of the skin due to the profuse proliferation of mites resulting from an altered host response to the infestation. Various cutaneous, neurologic and immunologic diseases have been described to predispose to crusted scabies [Table - 1]. [3] Most of the reports are anecdotal case reports and only a few case series of crusted scabies exist in the literature. [4],[5],[6] Etiology The causative agent is the scabies mite, Sarcoptes scabiei var hominis . The mite is an obligate parasite that lives in burrowed tunnels in the stratum corneum. The female mite, the chief culprit, is about 400 microns in length and has a rounded body with four pairs of legs. The front two pairs end in "suckers" and the hind two pairs in long trailing bristles. [7] In the skin, the mite survives on a diet of dissolved human tissue but does not feed on blood. It makes burrows of about 0.5-5mm in the stratum corneum every day. The mite lives in the burrow for a period of 30 days. The female lays two-three eggs daily and the eggs hatch in 3-4 days. The young larva passes through the nymphal stage to the mature adult mite stage in 14-17 days. It is estimated that only 10% of the eggs develop into adults. The average mite in normal patient is 11. [8] However, in case of crusted scabies, the number of mites is astronomical because of uncontrolled proliferation. The incubation period before the onset of symptoms is 3-6 weeks for primary infestation, but may be as short as 1-3 days in reinfestation. Pathogenesis The cutaneous manifestations of scabies are due to the burrowing of the female mite in the stratum corneum and stratum malpighi followed by humoral and delayed hypersensitivity. [9] The mite antigens that trigger the immune response are probably in the saliva. Combined with scratching, the immune system in the healthy host will reduce the mite load but rarely eliminates the mite. The failure of the immune system to suppress the proliferation of the mite is an important cause of crusted scabies development. Crusted scabies typically develops in patients with a defective T-cell immune response or decreased cutaneous sensation and reduced ability to mechanically debride the mites. Crusted scabies also develops in Australian aborigines with normal immunity. [10] The reason for the occurrence of crusted scabies in this community is unclear. Certain studies have shown an association between scabies and HLA-A11. [11],[12] Hyperkeratosis of the skin, which is a prominent feature in crusted scabies, is probably related to increased levels of interleukin-4. [12] Recent studies have shown that skin-homing cytotoxic T cells contribute to an imbalanced inflammatory response in the dermis of crusted scabies lesional skin. This, in combination with the lack of B cells, results in failure of the skin immune system to mount an effective response, resulting in uncontrolled growth of the parasite. [13] Transmission Scabies is a highly contagious disease. The predominant route of transmission is skin-to-skin contact. Transmission via fomites is more commonly seen in crusted scabies. The immediate environment of a patient with crusted scabies is heavily infected with mites. Patients with crusted scabies are capable of triggering an epidemic of scabies. [6] Clinical Features Crusted scabies is a severe variant of highly contagious scabies. Itching, which is a hallmark of scabies, is minimal or absent. It is generally believed that patients with crusted scabies do not itch. But, at least 50% of the patients have some degree of itching. [6] The itch, if present, diminishes with time. Crusted scabies usually do not present as an acute eruption as in classical scabies. The eruption is slow in onset and insidious in progression. There are two principle components - localized horny plaques and a more distinct erythematous appearance. The plaque is composed of a parakeratotic crust that varies in thickness from about 3 to 15mm [Figure - 1],[Figure - 2],[Figure - 3]. The crusts are creamy, grey, yellow brown or yellow green in color and are adherent and firm but, when removed, they have a porous appearance resembling a pumice stone. The lesions found over the extensor surface show fissuring. When the lesions are very large and thick, the whole surface may be broken up into slabs by these fissures. On removal of the crust, the undersurface is smooth, red, moist and velvety in appearance. Such crusts are seen over the palms, on the extensor aspect of the elbows, on the scalp and ears and on the soles of the feet and the toes. [6] Crusted scabies may also present as psoriasiform dermatitis. It can also present as warty dermatosis of the hands and feet with hyperkeratosis of the nails. The nails are dystrophic with abundant psoriasis like subungual hyperkeratosis and debris. The nails are the frequent source of relapse. Rarely, crusted scabies may involve the entire body, including the head and the scalp. This involvement may lead on to erythroderma. Sometimes, scabies can be localized to the scalp, penis, face, finger and soles. [6] An isolated report of crusted scabies presenting as bullous pemphigoid-like eruption exists. This patient also had crusted lesions elsewhere on the body. In such patients, an indirect immunofluorescent study is important to distinguish between scabies with blister formation and true bullous pemphigoid. [16] Complications Crusted scabies is complicated by secondary bacterial infection by Staphylococcus aureus . They include impetigo, ecthyma, cellulitis and lymphangitis. [6] Generalized lymphadenopathy is another important complication. Rarely, septicemia may occur in these patients. Differential Diagnosis Crusted scabies can mimic a variety of conditions, [17] such as:
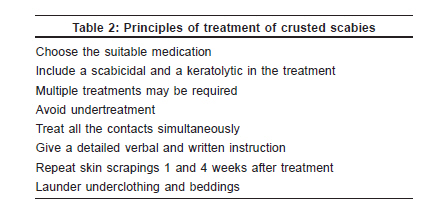
Diagnosis Diagnosis is based on clinical findings and the demonstration of the mite. Microscopic examination of the skin scrapings from the patient is essential to demonstrate the mites. The specimen from the crusted lesion is scraped with a blunt scalpel and placed on a glass slide. A drop of mineral oil and a cover slip are placed on it. The microscopic examination reveals numerous mites, eggs and mite feces (scybala). Demonstration of mites, eggs and mite feces (scybala) is diagnostic of scabies. [5] Epiluminescence microscopy and high-resolution videodermatoscopy are noninvasive techniques that allow a detailed inspection of the patient′s skin, from the surface to the superficial papillary dermis, and can be used to visualize the mite. [34],[35] Further, standard dermoscopy is a useful tool for diagnosing scabies, with a high sensitivity, even in inexperienced hands. [36] Histopathology can be diagnostic if mites or parts of the mite are identified in the section. Eosinophilia is found in 58% of the affected patients. The median immunoglobulin E levels were elevated in patients with crusted scabies in contrast to scabies. [37] The DNA finger printing system for Sarcoptes scabiei , through the polymerase chain reaction technique, is useful in crusted scabies to determine whether the patient is really cured or is getting reinfested. Further, an outbreak of scabies in the family members and close contacts gives a clue to the diagnosis. Any crusted lesion in a moribund or debilitated patient should be examined for Sarcoptes scabiei . Histopathology of crusted scabies The mites can be seen in all stages of development: Adult, larval, nymph and egg. Foci of spongiosis, spongiform pustules and neutrophilic abscess are seen in the spinous zone. A dense superficial and deep perivascular infiltrate of numerous plasma cells are seen in the dermis. Eosinophils and neutrophils are seen around the blood vessels at all levels of the dermis, especially the upper half. [39] Treatment It is important to strictly isolate patients with crusted scabies as these patients can easily trigger an outbreak of scabies. The household contacts or hospital staff should be instructed to take adequate precautions to avoid getting infested. The nails of the patients should be clipped and scabicidals should be applied as nails are the frequent source of relapse. Adequate care should be given to moribund or paralysed patients to prevent relapse. Their clothes should be laundered. The principles involved in the treatment of scabies are given in [Table - 2]. Treating crusted scabies can be very challenging due to various factors such as host′s compromised immunity, widespread nature of the eruption, the high mite burden and the limited penetration of the topical agents into the hyperkeratotic lesion. Thus, the treatment of crusted scabies not only includes scabicidals but also keratolytic agents to remove the thick crusts, which are a nidus for the mite. In crusted scabies, hyperkeratotic crusts prevent the adequate penetration of topical scabicidals. Removal of these crusts can be performed by employing a keratolytic agent such as 5-10% salicylic acid in petrolatum, 40% urea or by soaking in a hot bath. This may bring down the mite load and also enhance the efficacy of topical scabicidals. [40] Symptomatic treatment includes antihistamines for pruritus and an emollient for dry skin. Crusted scabies can be complicated by secondary bacterial infection. If septicemia occurs, it should be aggressively treated with broad-spectrum antibiotics. Various topical agents and oral drugs used in the treatment of classical scabies are also used in treating crusted scabies. Repeated applications are usually required and clearing is slower compared with ordinary scabies. The sequential use of two or more different agents or a combination with an oral agent may be necessary. Several drugs have been in use to treat crusted scabies, including topical sulfur compounds, benzyl benzoate, crotamiton, lindane, malathion, permethrin and ivermectin. [41] The use of lindane is contraindicated due to increased percutaneous absorption and the risk of neurotoxicity following repeated application. [42],[43] Topical permethrin, a synthetic pyrethroid formulation in a 5% cream, is presently the preferred topical scabicidal agent. [44] Benzyl benzoate Permethrin One major problem encountered with the use of topical scabicidals is that they require repeated application. Moreover, their efficacy, tolerability and specificity for crusted scabies are not well studied. Further, in patients with crusted scabies, the skin damage clearly attenuates the barrier function and poses a major toxicity risk if lindane is used. Hence, lindane should be avoided in crusted scabies. Permethrin is a good alternative, but requires repeated application. All these problems with topical antiscabietics can be avoided by the use of oral Ivermectin. Ivermectin Although it is lethal in mites, it is safe in human as it does not cross the intact blood brain barrier. The toxic effect of ivermectin appears to be insignificant. Ivermectin is contraindicated in a patient with an allergy to ivermectin and central nervous system disorders. Ivermectin has been used successfully in crusted scabies both as monotherapy or in combination with other scabicidals. [50],[51],[52] Although a single dose may be effective, many patients require two-three doses at an interval of 1-2 weeks. [53] This is because ivermectin has no residual drug activity against the parasite and treatment should be repeated if signs and symptoms recur. [54] Roberts et al . used a five-dose regimen to treat patients with crusted scabies. [55] Ivermectin was administered on days 1, 2, 8,9 and 15, with additional two doses on days 22 and 29 in most severe cases. With this regimen, he observed a significant decrease in patient mortality. Combination therapy Methotrexate was tried in the treatment of crusted scabies. [58] The use of methotrexate in crusted scabies is more of a historical interest rather than a recommended modality of treatment, with the advent of less-toxic and more-specific drugs such as ivermectin. Environmental Decontamination Normally, scabies does not require an environmental decontamination. But, patients with crusted scabies present a unique scenario. Their crusts, teeming with mites and laden with viable eggs, are constantly shed into the environment. A population density of 6312 mites/g was demonstrated in the dust from the linen.[59] These patients should be considered a hazard to others and appropriate isolation techniques should be adopted. It has been seen on several occasions in nursing homes that the hospital staff become infected by changing bedding and mattress. Gloves and gowns should be used while changing the bedding. Clothes and bed linen can be decontaminated by washing at 60°C. The use of insecticidal powder or aerosol should be reserved for materials that cannot be washed. [60] Prophylactic treatment of contact may involve an entire institution or visitors and family members. [59]Crusted Scabies And an Outbreak of Scabies Patients with crusted scabies can trigger endemic outbreaks of common scabies. Crusted scabies in elderly hospitalized patients can trigger an epidemic. Further, preexisting dermatosis, such as atopic or contact dermatitis, and use of topical steroids may mask the symptoms and promote transmission. The high potential of transmission of crusted scabies can be explained by the recovery of mites of all stages from the furnishings. Further transmission of mites may take place by the staff in old age homes. In case of a hospital outbreak, the index case is identified and started on treatment. All other patients in the ward and the staff should be treated simultaneously. The staff attending the patient with crusted scabies should wear gloves and a gown and avoid skin-to-skin contact. In contacts, permethrin 5% cream is used as first line followed by lindane and oral Ivermectin as third line. Human Immunodeficiency Virus and Crusted Scabies Scabies is commonly seen in HIV-infected patients. The defining clinical features are determined by the degree of immunosuppression. As the patients become more immunosuppressed, the more fulminant and contagious forms of scabies appear. These severe and unusual forms can be divided into papular and crusted scabies. Crusted scabies in acquired immunodeficiency syndrome (AIDS) patients can be manifested in both typical and atypical forms. Although the classic, hyperkeratotic, nonpruritic lesions are most common, reported cases have ranged in spectrum from crusting with pruritus to a pruritic, papular dermatitis to those resembling Darier′s disease or psoriasis. [61] Crusted (Norwegian) scabies usually occurs in patients with advanced HIV disease. [61],[62],[63] Although there are no definite studies to show the increase in the incidence of crusted scabies with the advent of HIV disease, a case series of crusted scabies from Dakar showed that HIV infection was the most commonly associated disease, seen in 45% of the patients. [5] Crusted scabies superimposed on psoriatic erythroderma, particularly in patients with AIDS, can pose both diagnostic and therapeutic challenges.[64] But, the presence of atypical crusted lesions and scrapping of the lesion is always diagnostic. Further, crusted scabies should always be suspected in any crusted lesion in AIDS patients. In these patients, ivermectin and permethrin are found to be effective in treatment. In patients with AIDS, crusted scabies can act as a portal of entry for the bacteria and lead to sepsis and death. [62] Conclusion Diagnosis and treatment of crusted scabies poses new challenges in the HIV era. Early diagnosis and proper treatment is the cornerstone to therapy. Ivermectin is the systemic drug of choice and repeated treatment may be required. But, no standardized protocols are available for treatment of crusted scabies. Further controlled double-blinded studies are needed to determine the best method of treatment. Future research is required to exactly understand the pathogenesis of the disease and the host-parasite interaction. Till then, crusted scabies cases will continue to occur and trigger epidemics of scabies. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09115f3.jpg] [dv09115t2.jpg] [dv09115f2.jpg] [dv09115f1.jpg] [dv09115t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}