 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
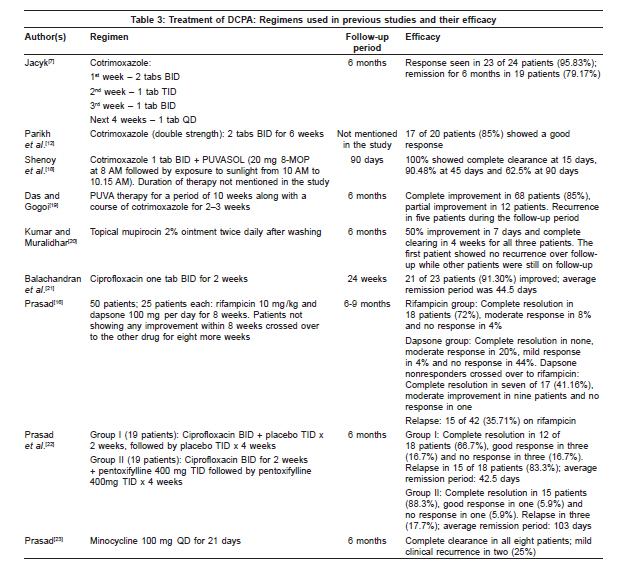
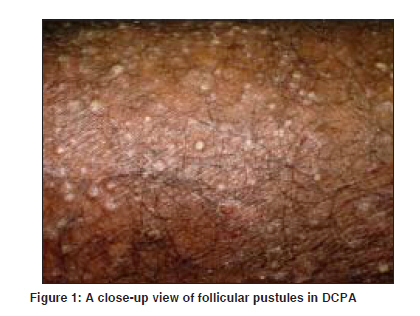
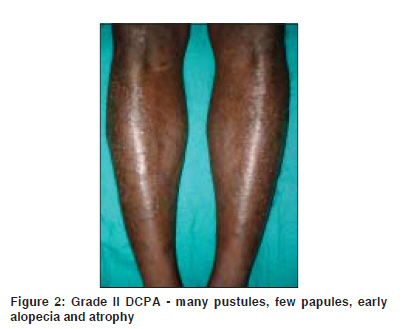
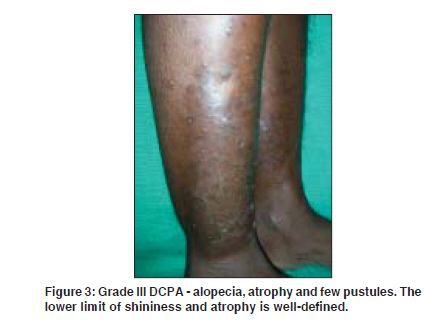
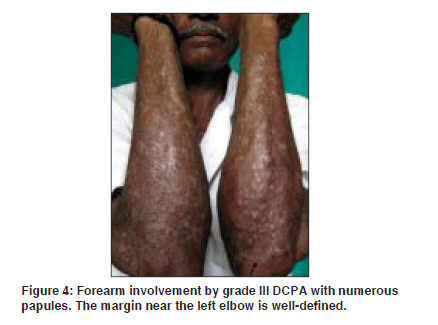
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 348-355 Review Article Dermatitis cruris pustulosa et atrophicans Kaimal Sowmya, D'Souza Mariette, Kumari Rashmi Department of Dermatology and STD, JIPMER, Pondicherry - 605 006 Code Number: dv09142 PMID: 19584458 Abstract Dermatitis cruris pustulosa et atrophicans (DCPA) is a distinctive type of chronic superficial folliculitis, primarily affecting the lower limbs. It is characterized by symmetrical follicular pustules of both legs, with cutaneous edema, resulting in alopecia, atrophy and scarring. It was first described by Clarke, from West Nigeria, in 1952 and well illustrated in his book "Skin diseases in the African," under the initial label of "Nigerian shin disease." Subsequently, it was described in India as well, in 1964, and continues to be a problem in dermatology clinics across the country. It is predominantly a disease of men and has a high prevalence in some geographical regions; up to 3-4% in Madras, South India. Some unique features that distinguish DCPA from banal pustular folliculitis include its peculiar localization to the legs, extreme chronicity, resistance to therapy and inevitable alopecia and atrophy of the involved skin, with little postinflammatory hyper- or hypopigmentation. Further, even in the presence of extensive lesions, there are no systemic features. Coagulase-positive Staphylococcus aureus is known to have a role in the etiology of DCPA, but the exact etiopathogenesis still needs to be elucidated. Immunological postulates such as hypergammaglobulinemia have been put forward to explain the chronicity of the condition. A number of therapeutic agents have been tried in various studies, including cotrimoxazole, psoralen with ultraviolet A (PUVA) therapy, ciprofloxacin, pentoxifylline, rifampicin, dapsone, minocycline and mupirocin (topical) with variable success rates. Although a well-recognized entity in dermatology clinics in tropical countries, DCPA has received little attention in the dermatological literature and has only a few studies to its credit. Its unique clinical picture, unclear etiopathogenesis and resistance to therapy afford a vast scope for further investigation and study. Keywords: Chronic folliculitis, Dermatitis cruris pustulosa et atrophicans, Staphylococcus aureus Introduction Pyodermas are common purulent infections of the skin caused mainly by Staphylococcus aureus and Streptococcus pyogenes . [1] Primary pyodermas may be follicular or nonfollicular. The common causes of superficial folliculitis are S. aureus , coagulase-negative staphylococci and physical or chemical irritation. S. aureus is among the most important causes of skin infections and serious, sometimes fatal, systemic disease. [1] Folliculitis of the skin may be superficial or deep, as in pyodermas caused by pyogenic organisms like S. aureus or due to other factors like irritation or occlusion. However, there are a number of inflammatory diseases involving the hair follicle, the etiology of which are complex or uncertain, with the role of bacterial infection being partial, secondary, not known or absent. For example, these include,conditions such as sycosis barbae and folliculitis decalvans. [1] Dermatitis cruris pustulosa et atrophicans (DCPA) is a distinctive type of chronic superficial folliculitis, of complex etiology, seen primarily in tropical countries. It primarily affects the anterior shins, with recurrent crops of itchy follicular pustules, which resolve either spontaneously or with treatment, resulting eventually in atrophy and loss of hair over the affected skin. The disease typically responds to a variety of topical and systemic antibiotics, but is characterized by recurrences that may be triggered by a variety of factors. Thus, DCPA has several unique features that distinguish it from banal pustular folliculitis, such as its peculiar localization to the legs, extreme chronicity, resistance to therapy and inevitable alopecia and atrophy of the involved skin, without any systemic symptoms. [2],[3] Historical Perspective Follicular diseases resulting in permanent alopecia and scarring have been known to physicians for over a 100 years. In the last century, French dermatologists described a number of these conditions under various names: pseudopelade (Brocq, 1885), folliculitis decalvans (Quiqaud, 1888) and acne decalvante (Lailler, 1884). [2] DCPA first earned a mention under the terminology "epilating folliculitis of the glabrous skin," described by Arnozan and Dubreuilh as "therapy-resistant symmetrical follicular pustules of both legs resulting in alopecia, atrophy and scarring." Although many such cases were reported in the European dermatological literature, it was an English dermatologist, Clarke, who is credited with describing a similar condition in the dark-skinned Africans of Nigeria. He coined the term "Dermatitis Cruris Pustulosa et Atrophicans" in the year 1952. [2] Miller described the first case from North America in 1961. However, he suggested the name "Lupoid Sycosis of the legs." [2] In India, Desai et al ., [4] in 1966, studied what they called "therapy-resistant pyogenic folliculitis of the legs" in 30 patients. Subsequent studies by the same authors showed these cases to be identical to DCPA. However, they also reported the occurrence of immunological abnormalities in these patients in the form of hypergammaglobulinemia. Harman, [3] in 1968, reviewed DCPA and studied it extensively among 15 outpatients in the Ibadan province of Nigeria. He gave a detailed clinical description of the lesions of DCPA, calling it the "Nigerian shin disease." He noted that although S. aureus was isolated from the lesions, they were uniformly resistant to antibacterial agents. He also suggested that the traditional practice of applying vegetable oils, especially coconut oil, may be an essential causative factor. In India, the disease has been termed "chronic folliculitis of the legs" (CFL) by Prasad et al . [5] The disease has thus acquired various names over the years, including "Nigerian shin disease," [3] "lupoid sycosis of the legs," [2] "therapy-resistant pyogenic folliculitis of the legs," [4] "folliculitis cruris pustulosa et atrophicans" [2] and CFL. [5] Epidemiology There is very little published epidemiological data on DCPA. As only hospital-based data are available, it serves at best as an approximate guide to the incidence of the disease in the community. DCPA is fairly commonly encountered in outpatient clinics in humid tropical climates. Shrank and Harman [6] reported a frequency of 2.2% in the Ibadan province of Nigeria from 1961 to 1963, while the Figure in a skin clinic in Kaduna, Northern Nigeria, was 4.8% among all outpatients in 1974. [7] However, a recent study from another skin clinic in Kaduna, Nigeria, reported a reduced frequency of DCPA (0.4%). [8] DCPA was reported to occur in 3-4% of dermatology outpatients in Madras, South India, while the corresponding Figure was 2.9% in Matara, Sri Lanka. [9] In general, DCPA is seen primarily in West Africa, Trinidad, India and Malaysia, whereas no definite cases have been reported after Miller′s original report in 1961 from any part of the United States or Europe till date. [3] DCPA is a disease predominantly of males, [2],[9],[10] although some studies have reported an equal incidence in males and females. [3],[7],[11] Males constitute anywhere between 50 and 91% in various studies.[2],[7] Although it has been reported to occur up to the sixth decade, [2] it is largely a disease of the second to third decade. [2],[3],[9],[11] The disease is invariably chronic, the duration lying anywhere between a few months to 22 years, [2],[5],[12] with some studies reporting a duration of 1-2 years in the majority of their patients. [5],[7] Sugathan et al . found that a third of their patients had a disease duration greater than 5 years. [2] Clinical Features of DCPA The main features of the eruption are shown in [Table - 1]. [2],[3] The general health is not affected and there is a notable absence of systemic symptoms such as fever as well as regional lymphadenopathy, even in the presence of extensive lesions. The state of nutrition and hygiene is usually satisfactory. [2],[3] Some Indian studies have noted a unilateral onset of disease in 25-75% of the patients. [2],[12] Among these patients, the time taken for the involvement of the other leg varied from 1 month to 8 years. [2] The degree of pruritus in DCPA ranges from mild to severe. It may be the most prominent and distressing symptom in some, [5],[13] while it is common but mild in others. [9] Pruritus may persist even after resolution of the lesions and sudden onset of pruritus may be a marker of relapse. [5] Invariably, the eruption begins on the lower third of both legs. The borders are well defined, especially the lower margin, which is very sharp, but conforms only approximately to the lower limit of the terminal hairs at the ankle. [3] Even in advanced cases, some totally unaffected hair follicles can be seen on the ankle distal to the eruption. The dorsa of the feet and other areas of glabrous skin are never affected. [3],[12] Sugathan et al .[2] observed in their study that 52% of patients had involvement of the front of the thighs as well. Also, involvement of the forearms (22.8%) and the face (3.8%) was noted by them among Indian patients. The trunk, scalp and pubic region were never affected. [2],[3] Some other studies have also recorded involvement of areas other than the legs, such as the thighs and forearms, ranging from 13.7 to 35% of the cases. [3],[5],[7],[9] Nearly all follicles in the affected area contain a pustule, from the center of which a single hair can be seen to be emerging. The leg usually becomes scaly and shiny, with a variable amount of pitting edema. Normal skin marking is lost and there is some atrophy. [2] In long-standing cases, the direction in which the terminal hairs emerge is haphazard such that running the fingers lightly over them gives a sensation of wiry roughness.[3] Also, with chronic cases, there may be a reduction in hair-bearing follicles and the remaining hair may also be short and irregular. The disease may undergo a natural cure once all the hair in the affected area is lost. [9] Further, in contrast to many inflammatory dermatoses, there is little postinflammatory hyper- or hypopigmentation.[2] However, one study from Sri Lanka did record postinflammatory hyperpigmentation. [9] Eczematous changes have been described in a few patients, whereas in others, signs and symptoms such as minimal pain, burning, oozing, bleeding and scaling have been seen. [5],[9] The individual manifestations of the condition vary from case to case and in the extent to which they dominate the clinical picture. Pustular folliculitis, scaling, shiny edema and follicular atrophy with scarring may each be the major feature in different patients. Owing to this pleomorphic dominant picture, Sugathan et al . [2] suggested a clinical grading for DCPA [Table - 2]. Thus, DCPA has a number of peculiar clinical features that justify its status as a distinct clinical entity: The appearance of follicular pustules associated with pruritus, symmetrically localized to the legs, leading to alopecia and atrophy, with occasional, although rare, involvement of the forearms, face and scalp; the trunk and pubic region never being affected in spite of these sites fulfilling the prerequisite of possessing well-developed terminal hair. Aggravating Factors Subjective and objective aggravating factors have been reported in most studies. In early studies by Harman in Ibadan, application of vegetable oils, especially coconut oil, was considered an essential causative factor. [3] The application of oil for cosmetic or medicinal purposes is a common practice in Western Nigeria, where four types of oils are commonly used, namely, coconut oil, palm oil, palm kernel oil and shea butter.[3],[11] In India, coconut oil and mustard oil are commonly used. [12],[13] Jacyk suggested that occlusion, leading to increased hydration of the stratum corneum, makes DCPA worse because moist skin has a higher friction coefficient than dry skin and is hence more vulnerable to trauma. [11] Sugathan et al . reported a wide variety of factors, including the ingestion of animal protein, consumption of alcohol, sleeplessness, excessive sweating and contact with wet soil and cowdung. [2] They, however, found that application of coconut oil did not in any way influence the course of the disease, a finding similar to that of Desai et al . in another study. [4] Some patients who came in contact with oil at the work place (cooks, drivers, mechanics) reported improvement during leave at home. [13] Later studies pointed out that while oil application was all over the body, lesions were localized to the lower limbs. Also, patch and usage tests with coconut and mustard oil were negative. [12] Allergic contact dermatitis to topically applied antibacterial agents has been postulated as a perpetuating factor for the folliculitis. [12] Physical or chemical injury may also precipitate this condition, a possibility reflected by the finding that most of the patients were farmers in one Indian study by Prasad et al . [5] In another study, most patients were sugarcane harvesters and they attributed the cause of their folliculitis to the stiff needles on the bark of the sugarcane. [10] Although patients may be from diverse walks of life, [4],[7] outdoor work [10] is an important predisposing factor. A field survey of epilating folliculitis among fishermen in Calicut, Kerala, [14] revealed an incidence of 20.4%, which is much higher than that reported in the general population. Constant wetting of the skin with sea water was considered an important predisposing factor. [14] Additional relevant etiologic factors may be scrubbing of the legs with rough objects like pumice stones, ichthyosis and occupational exposure to irritants. [9],[11] The disease shows a pronounced seasonal variation, with most exacerbations occurring in the summer and monsoon months. [2],[11] Conditions known to be associated with resistant pyogenic infections, such as diabetes, malnutrition, tuberculosis and malignancy, have not been found in patients with DCPA. [2],[4],[11] Immunological Abnormalities One of the most important features of the disease has been its striking chronicity, with disease duration of up to 22 years being reported. [2] This would seem to suggest an underlying immunological mechanism. As early as 1969, Desai et al . [4] had reported the occurrence of hypergammaglobulinemia in 30 patients. Sugathan et al . [2] further found that the presence of hypergammaglobulinemia had no correlation with the extent of involvement or duration of illness and, therefore, reflected only the presence of a chronic infection. Subsequent investigations by Tiwari et al . [13] in 15 soldiers showed that immunoglobulin (Ig) G was increased in all cases. The levels varied from 1650 to 1973mg/100 ml. IgA was marginally increased in 20% of the cases, while no increase in IgM was seen. [13] A systematic study was undertaken by Parikh et al . [12] to address the various lacunae in the immunology of DCPA. They studied polymorphonuclear (PMN) percentage phagocytosis, intracellular killing (ICK) capacity and Ig and complement levels in 20 patients. They found that both the parameters of PMN function, i.e. percentage phagocytosis and ICK, were significantly raised above normal in the initial stage and returned to normal after treatment, suggesting that there was no abnormality of PMN function. There was no significant rise in the Ig levels, suggesting a depressed immunological response. Further, they found that C3 levels were also decreased. They felt that these two factors could play a decisive role in the chronicity of this condition. However, these findings are in contrast to earlier studies. Hence, more studies are needed to clarify the immunological role in the etiopathogenesis of this enigmatic condition. Microbiology of DCPA All studies on DCPA have shown primarily isolates of S. aureus from the pus cultures, making it virtually the prime pathogen responsible for DCPA. [3],[11],[12],[13] Additional bacteria that have been grown in culture from DCPA pustules in a small percentage of cases include Pseudomonas spp., Klebsiella spp. and beta hemolytic Streptococcus. [5],[15] Although Trichophyton rubrum has been considered by some authors as a possible pathogenic agent, no evidence to support this theory has been documented. [3] In an early landmark study by Harman, swabs from two-thirds of the patients grew S. aureus, of which half were penicillin resistant. [3] In three patients, S. aureus was grown from nasal swabs as well. However, no link was established between the nasal and leg pustule flora. Phage typing of staphylococci from 12 cultures from the same series showed a heterogeneous collection representative of organisms typically found as secondary invaders in lesions due to some other cause, similar to any skin department in Britain. [1] Tiwari et al . [13] isolated S. aureus from pustular lesions in all their patients; however, a majority (87%) were resistant to penicillin but sensitive to erythromycin, chloramphenicol, ampicillin and other antibiotics. Similar results were also obtained by Parikh et al ., who studied 20 patients of DCPA and isolated S. aureus from all their pus samples. [12] Predictably, all strains were resistant to penicillin but sensitive to erythromycin, chloramphenicol and cotrimoxazole. Histopathology of DCPA Some authors consider DCPA a combination of superficial and deep folliculitis, [1] while others are of the opinion that inflammatory changes are confined to the ostium or slightly below it and healing correspondingly occurs without scar formation. [16] The epidermis shows mild to moderate hyperkeratosis and parakeratosis in loose bands of stratum corneum.[13] Findings in early lesions include only nonspecific focal round cell infiltration of the dermis and focal infiltration of the mouth of the hair follicle by polymorphs. [2] Intraepidermal and subcorneal pustule formation containing leukocytes is seen, [4] with adjacent areas of the skin heavily infiltrated by neutrophils, lymphocytes and occasional eosinophils. Well-developed pustular lesions show a "wine glass"-shaped abscess involving the upper part of the hair follicle without involvement of the bulb or root of the hair [Figure - 5]. The hair shaft can be seen passing through the abscess cavity. [2] Some of the pustules in grade I and II disease were found to be unassociated with hair follicles in one study by Jacyk. [11] Flakes of keratin and acantholytic cells can also be seen in the abscess cavity. Lymphocytic and plasma cell infiltration of the sweat glands and hair follicles can also be seen. There is, however, an absence of foreign body giant cells. [2] Another notable feature is the presence of marginal acanthosis around the abscess. [2],[3] A recent report noted the histopathologic presence of an intraepidermal neutrophilic pustule along with eosinophilic cellulitis and panniculitis with flame Figures in a female patient with lesions of both DCPA and prurigo nodularis. [17] In the cicatricial stage, the rete ridges are atrophic, with atrophy of the appendages, upper dermal fibrosis and focal collection of round cells around the appendages.[11] Additional epidermal and dermal changes that have been described include hyperkeratosis, parakeratosis, acanthosis, spongiosis and occasional red blood cell-containing vesicles. [2],[3] Treatment of DCPA Treatment for this condition is unsatisfactory, leading to the usage of the term "therapy-resistant folliculitis." Both Harman and Sugathan, in their studies, have remarked about the resistance to various systemic and topical therapies. [2],[3] Modalities of therapy for DCPA that have been studied include systemic and topical antibacterial agents (cotrimoxazole, ciprofloxacin, rifampicin, dapsone, minocycline, topical mupirocin), pentoxifylline and PUVA. [Table - 3] shows a summary of the treatment regimens used for DCPA in various studies. Ultimately, combination therapy with antiseptic lotions, long-term systemic antibiotics, topical antibiotics and avoidance of risk factors are essential in controlling the disease. However, the disease is generally refractory to most forms of therapy and it is difficult to halt its inexorable progression to alopecia and atrophy of the affected site. Conclusion Although a common entity, DCPA has received little attention in dermatological literature and has only a few studies to its credit. Its unique clinical picture, unclear etiopathogenesis and resistance to therapy afford a vast scope for further investigation and study.[23] [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4]References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09116f3.jpg] [dv09116t1.jpg] [dv09116f4.jpg] [dv09116f5.jpg] [dv09116t2.jpg] [dv09116f2.jpg] [dv09116f1.jpg] [dv09116t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}