 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
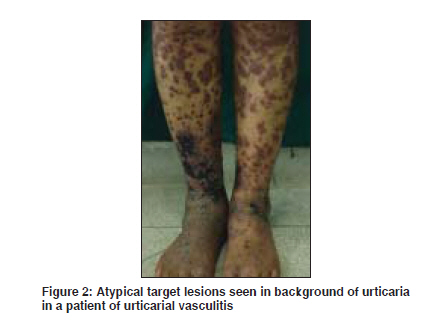
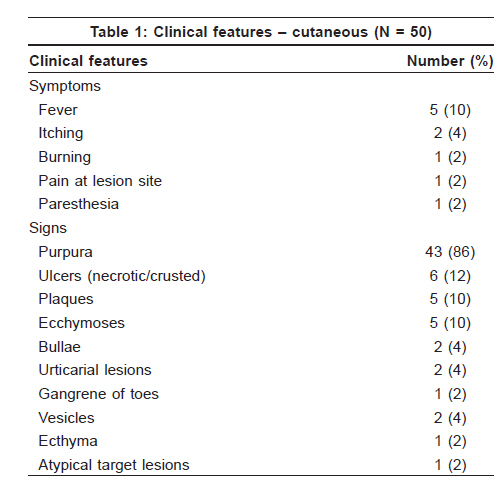
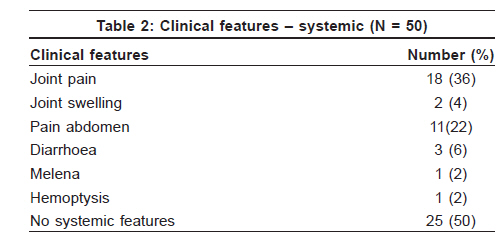
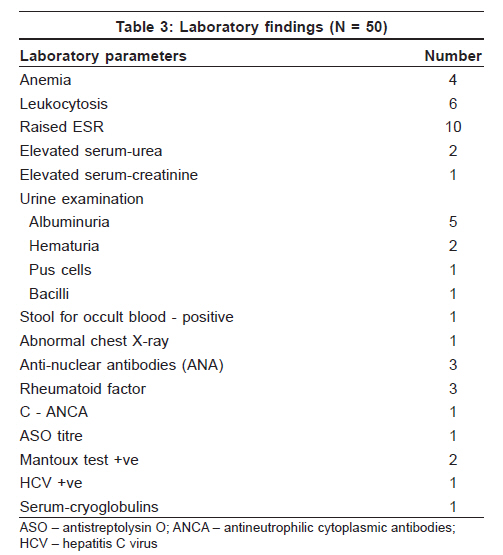
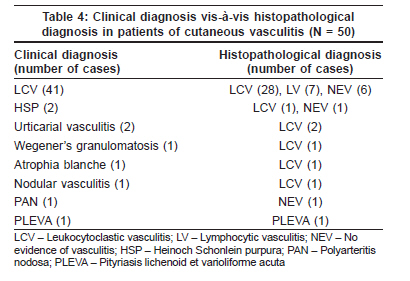
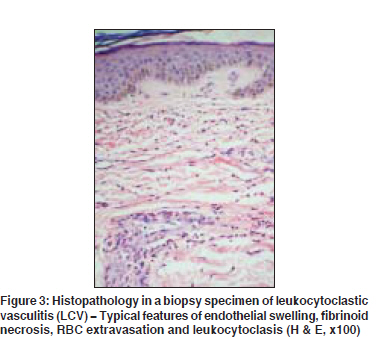
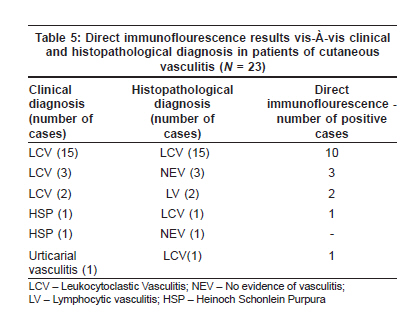
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 356-362 Original Article Cutaneous vasculitides: Clinico-pathological correlation Gupta Suruchi, Handa Sanjeev, Kanwar AmrinderJ, Radotra BishanDass, Minz RanjanaW Departments of Dermatology, Venereology, Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh Code Number: dv09143 PMID: 19584459 Abstract Background: Cutaneous vasculitis presents as a mosaic of clinical and histological findings. Its pathogenic mechanisms and clinical manifestations are varied. Keywords: Cutaneous vasculitis, Skin biopsy, Direct immunoflourescence Introduction Vasculitis is an inflammation of the blood vessel wall and it can have a wide range of clinical manifestations. Most reviews on vasculitides have been written from rheumatologist′s perspective. [1],[2] The skin is commonly involved in systemic vasculitic disorders, and cutaneous vasculitic lesions offer a window to diagnosis and a ready source of accessible tissue for histopathologic examination. Many times the initial presentation of vasculitis is on the skin and it is the dermatologist who must diagnose and treat this challenging condition. The classification of vasculitis is controversial with no generally accepted classification system. The classification systems of the American College of Rheumatology (ACR) and of the Chapel Hill Consensus Conference (CHCC) have gained wide acceptance. Yet, they need to be updated, especially with regard to leukocytoclastic vasculitis (LCV), the most common vasculitis of the skin. [3] Despite the best efforts at diagnosis, no identifiable cause is found in nearly one-third patients of vasculitis. Cutaneous vasculitis presents as a mosaic of clinical and histological findings due to varied pathogenic mechanisms. [4],[5] A definitive diagnosis of vasculitis requires histological confirmation in almost all cases because few vasculitic syndromes have pathognomonic clinical, radiographic and/or laboratory findings.[6] However, histopathologic diagnosis alone cannot stand by itself and must be correlated with clinical, physical and laboratory findings. Our study was an attempt to understand the epidemiological spectrum of cutaneous vasculitides as seen in a dermatologic clinic and to determine the clinico-pathological correlation. Methods A cohort study was conducted on 50 consecutive patients clinically diagnosed as cutaneous vasculitis in dermatology outdoor clinic of our hospital, from September 2004 to March 2006. All patients with clinical evidence of cutaneous vasculitis, irrespective of age, sex and duration of the disease were enrolled in the study. Patients presenting with simultaneous crops of palpable purpura, papules, plaques, nodules, vesicles, bullae, pustules, ulcers and other cutaneous findings like urticaria, livedo reticularis or edema were included in the study. Based on the clinical presentation, an attempt was made to classify vasculitis as per updated Gilliam′s classification. [7] The patients with thrombocytopenia (< 50, 000/mm 3 ) and disorders of coagulation; and patients on warfarin/heparin and patients with age of last appeared lesion more than 48 h were excluded from the study. A detailed history and clinical examination were carried out in all patients. History of drug exposure was considered significant if exposure was within 8 weeks of appearance of lesions. Baseline investigations - complete hemogram, erythrocyte sedimentation rate (ESR), serum-urea and serum-creatinine levels, liver function tests, chest X-ray, urine (routine and microscopic) examination, stool for occult blood, antistreptolysin O (ASO) titer, Mantoux test, cryoglobulins, antinuclear antibodies (ANA), antineutrophilic cytoplasmic antibodies (ANCA), rheumatoid factor (RF) and markers for hepatitis B and C were done in all patients and specific investigations in select patients based on underlying disease etiology. Histopathological examination of a lesional skin biopsy specimen of the suspected vasculitic lesions was performed in all patients. Skin biopsy was taken under strict aseptic conditions, using 4 mm disposable skin punch. Sections were formalin fixed, paraffin embedded and stained by hematoxylin and eosin stain for light microscopic examination. Although specific histopathological features were dependent upon the type and size of blood vessel affected; however, vasculitis was broadly classified [4] as below in three main types: Leukocytoclastic vasculitis (LCV): Characterized by swelling of endothelial cells, fibrinoid necrosis of vessel wall, neutrophilic infiltration with leukocytoclasis and extravasation of RBCs. Patients fulfilling two out of four criteria qualified for a diagnosis of vasculitis Lymphocytic vasculitis: Characterized by perivascular lymphocytic cuffing and thickening of blood vessels. Granulomatous vasculitis: Characterized by palisading granulomatous inflammation around blood vessels. Direct immunofluorescence (DIF) was done in 23 patients. The immunofluorescence corresponding to immune complex deposits around dermal blood vessels was recorded arbitrarily as strongly positive (3+), moderately positive (2+) and weakly positive (1+). Statistical analysis Results A total of 50 patients clinically diagnosed as cutaneous vasculitis in dermatology outdoor clinic were enrolled in the study. There were 20 male and 30 female patients with age range of 5-67 years. The mean age of the study group was 41.1 years for males and 35.9 years for females. Palpable purpura was the commonest cutaneous presentation noticed in 43 patients (18 males and 25 females). The commonest sites of purpura were legs and ankles followed by thighs, buttocks, forearm, abdomen, back and chest [Figure - 1]. The other cutaneous lesions seen in 22 patients were in the form of plaques, ulcers, bullae, vesicles, ecthyma, gangrene of toes, urticarial lesions and atypical target lesions [Figure - 2]. The time since onset of lesions varied from 1 day to 9 months. There was history of similar cutaneous vasculitic lesions in the past in 9 (18%) patients. These findings have been summarized in [Table - 1]. Fever was the commonest presenting symptom in five patients and 2 patients complained of itching, while burning and pain at the site of the lesion and paresthesia in the legs were encountered in one patient each. Systemic involvement was encountered in 25 (50%) patients [Table - 2]. Associated joint pains were the commonest systemic presentation in 18 patients with knee joint being the most commonly involved joint (8 patients). Other joints involved were ankle joint and small joints of feet and wrists. Joint swelling was observed in 2 patients. There was history of pain abdomen in 11 patients, diarrhea in 3 patients and melena and hemoptysis in 1 patient each. Twenty five patients gave history of drug intake prior to the appearance of lesions. These included analgesics in nine, antibiotics in four, Ayurvedic medicines in two, Homeopathic medicines and contrast media during angiography, amlodipine, eltroxin, asthalin, interferon, neostigmine in one patient each and unknown drugs in two patients. While no significant past history was elicited in 38 patients, three patients gave history of essential hypertension and tuberculosis; atopy, cirrhosis, hepatitis C virus infection (HCV), chronic obstructive airways disease, diabetes mellitus, hypothyroidism, myasthenia gravis, nephrotic syndrome and superior sagittal sinus thrombosis was elicited in one patient each. The hematological and biochemistry workup [Table - 3] revealed anemia in four patients, leukocytosis in six, elevated ESR in ten, raised serum-urea in two and raised creatinine levels in one patient. Routine urine examination showed albuminuria in five patients, while urine microscopy demonstrated blood cells in two patients and pus cells and bacilli in one patient each. The stool for occult blood was positive in one patient. Smear culture from ulcerated lesion in one patient revealed growth of Pseudomonas aeruginosa. Anti-nuclear antibody and rheumatoid factor were positive in three patients each, while c-ANCA, Hepatitis C virus and serum cryoglobulins were positive in one patient each. ASO titer was also raised in one patient, while Mantoux was positive in two patients. Clinically, 41 (82%) patients were offered a diagnosis of LCV, 2 (4%) patients each of urticarial vasculitis and Henoch−Schonlein purpura (HSP). Wegener′s granulomatosis, atrophia blanche, nodular vasculitis, polyarteritis nodosa (PAN) and pityriasis lichenoides et varioliformis acuta (PLEVA) were diagnosed in one (2%) patient each. Based on histopathological findings, 34 (72%) patients were given a diagnosis of cutaneous small vessel vasculitis, 6 (12%) were diagnosed as lymphocytic vasculitis, 1 was diagnosed as PLEVA, while 8 (16%) patients did not show any evidence of vasculitis [Table - 4]. The skin biopsy showed typical features of endothelial swelling, fibrinoid necrosis, RBC extravasation and leukocytoclasis [Figure - 3]. Direct immunofluorescence examination results were available for 23 patients only, out of which 17 (73.9%) were found positive for the evidence of vasculitis. IgM and complement were the commonest deposits positive in 12 (52.2%) patients each. IgA was seen in 10 (43.5%) patients and IgG was the least common deposit seen only in 6 (27.1%) patients. In addition, faint lupus band and Civatte bodies were seen in 1 (4.3%) patient each. Trying to look into the etiological spectrum in our study [Figure - 4], 50% cases occurred following drug intake, infectious aetiology was suspected in 10% cases, collagen workup was positive in another 10% of patients though no overt collagen vascular disease was detected in any of these patients; WG and cryoglobulinemia were detected in 2% each. Malignancy was not detected in any of our cases and 26% of cases were found to be idiopathic. The results are depicted in [Figure - 4]. In 15 cases of LCV, where clinical and histological diagnosis were concordant, DIF was found positive in only 10 patients. While in three patients clinical diagnosis and DIF findings were consistent but histopathology did not show any evidence of vasculitis. In another two patients with clinical diagnoses of LCV, histopathological examination revealed lymphocytic vasculitis and DIF was found positive in both these patients. Amongst the two suspected cases of HSP, one did not show evidence of vasculitis on histopathology and DIF; while in the other case, histopathology revealed changes of LCV and DIF examination revealed vasculitis with deposition of IgA, IgM and complement. In one case of urticarial vasculitis where histopathological features revealed it as LCV, DIF showed all four immune complexes with predominant complement deposits. These findings are summarized in [Table - 5]. Discussion Cutaneous vasculitis is a poorly understood entity due to its protean clinical manifestation and its overlap with various infections, connective tissue disorders and malignancies. In our study, we analyzed clinical features, relevant past history and various laboratory tests to reach a clinical diagnosis of cutaneous vasculitis. An attempt was also made to classify the disease entities seen. The clinical diagnosis was confirmed by skin biopsy and DIF. Our study confirms various established facts regarding cutaneous vasculitis and throws light on some new aspects. A possible etiological association was suspected in 74% of our patients which was comparable to 67.2% seen by Sais et al . [8] Systemic involvement was observed in 50% and there was no mortality due to vasculitis in our study, unlike Sais et al ., who reported 2% patients dying of systemic involvement. The most common clinical presentation in our study was crops of nonthrombogenic palpable purpura, primarily involving dependent areas such as legs, ankles, feet and buttocks seen in 86% of patients. This was comparable with earlier studies by Sais et al . [8] and Ekenstam et al . [9] in 89.2 and 62% of cases, respectively. The second most common type of lesion in our study was cutaneous necrotic or crusted ulcers observed in 12% of patients. In comparison, Sais et al. [8] observed cutaneous ulcers in 20.3% of patients. Asymptomatic purpuric lesions were seen in 90% of patients in our study in contrast to Sais et al. [8] where 41.3% patients complained of pruritus and 30% patients had painful lesions. Fever was seen in only 10% of our patients while it was seen in 31.6% patients by Sais et al . [8] The history of similar cutaneous vasculitic lesions in the past could be obtained only in nine (18%) patients. Nine (18%) patients had persistent type of cutaneous lesions and out of these six had more than one type of lesions of which three had ulcerated lesions and three had joint involvement. Amongst patients who had systemic disease, cutaneous lesions were painless in all cases, necrotic and ulcerated in six and fever was present in three patients only. Systemic involvement was observed in 25 (50%) patients with joint pains being the commonest presenting manifestation in 18 (36%) patients. This was again in consonance with the systemic involvement observed by Ekenstam et al. [9] in 51% patients where musculoskeletal system was most commonly involved system in 43% patients. However Sais et al. [8] observed systemic involvement only in 20% of the cases with joint involvement in 36.7% of all cases. Gastrointestinal involvement was seen in 22% of our patients mainly in the form of pain in abdomen, diarrhea, frank blood and occult blood in stools in LCV, HSP and urticarial vasculitis patients, while it was seen in 9.5% cases by Sais et al . [8] Presentation with an acute abdomen is quite common (50−85%) in HSP and about one-third of these cases presented with gastrointestinal hemorrhage. [10],[11] Lanzkowsky et al. [12] have reported that 14% patients in their series had gastrointestinal symptoms preceding cutaneous lesions and diagnosis might become difficult in this situation. The interval between abdominal symptoms and appearance of skin lesions in such cases may vary from 2 to 24 weeks. [12],[13] Winkelmann and Ditto [14] found renal involvement in 61% of their patients, while in our study renal involvement was seen in only 16% of patients. In our study renal involvement was seen in WG and LCV; in the form of proteinuria and microscopic hematuria. In patients of LCV with renal involvement, three had extensive cutaneous lesions all over the body while three patients had musculoskeletal symptoms. Pulmonary involvement was seen in only one case in the form of hemoptysis and multiple cavities in a patient of WG. Pulmonary involvement was observed in 40% patients by Winkelmann et al. [14] and 8% patients by Ekenstam et al . [9] Hypertension was seen in 6% of our patients similar to 8.7% in the study by Sais et al . [8] Tuberculosis was seen in 6% of our patients in contrast to no case detection in study by Sais et al.[8] and Ekenstam et al . [9] This is probably due to the high prevalence of tuberculosis in India. Hepatitis C virus positivity was seen in only 2% of our patients in contrast to 21% by Sais et al . [8] Half of our patients had a recent history of drug intake with analgesics being the most commonly implicated drugs seen in 36% cases, while relevant drug history is reported in 10% of patients by Ekenstam et al. [9] with antibiotics being the commonest offending agents in 50% cases. The laboratory parameters reflecting systemic inflammatory responses were elevated ESR in 10 (20%) patients, anemia in 4 (8%) and leukocytosis in 6 (12%) patients. Sais et al . [8] observed elevated ESR in 52.4% patients, anemia in 37% and leukocytosis in 18%. The renal functions were altered in 3 (6%) patients in the form of elevated urea and creatinine and abnormal urine examination in 8 (16%) patients. Sais et al. [8] found these parameters to be 26 and 21.1%, respectively. Liver function tests were within normal limits in all patients while Sais et al. observed elevated transaminase levels in 18% of patients. The collagen vascular disease workup revealed positive ANA with speckled pattern and rheumatoid factor in 3 (6%) patients each, while it was observed in 28.5 and 26.4% patients, respectively, by Sais et al . [8] In addition, c-ANCA, HCV and serum cryoglobulins were found positive in 1 (2%) patient, ASO titer was raised in one (2%) patient, while Mantoux test was positive in two (4%) of our patients. Sais et al. reported serum cryoglobulins in 25.4% patients while c-ANCA and Mantoux test were negative, and ASO was not found raised in any patient. Histopathology showed features of vasculitis in 42 patients and additional 3 patients showed immune complex deposition on DIF, though histopathology was inconclusive in these 3 cases. For the remaining 5, the diagnosis of cutaneous vasculitis was considered on the basis of high index of clinical suspicion. Moreover, histopathology was noncontributory in these cases, probably due to the biopsy of the lesion at a late stage in the disease evolution. In summary, the workup of patients with suspected cutaneous vasculitis starts with a detailed history into possible etiological factors like drugs, recent infection and the presence of preexisting symptoms suggesting any underlying disease. A careful correlation of the medical history and the clinical, serological and imaging findings can help reach a correct diagnosis. However in all patients, skin biopsy and DIF are must for final diagnosis and accurate classification of vasculitis. [1],[15] However, these should be done at an appropriate stage of evolution of the disease, so as to avoid missing important diagnostic evidence despite strong clinical suspicion. And lastly a careful followup of these patients is mandatory as cutaneous manifestations might be just the forme fruste of serious systemic involvement. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09117t2.jpg] [dv09117f1.jpg] [dv09117t5.jpg] [dv09117f2.jpg] [dv09117t4.jpg] [dv09117f4.jpg] [dv09117t1.jpg] [dv09117f3.jpg] [dv09117t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}