 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
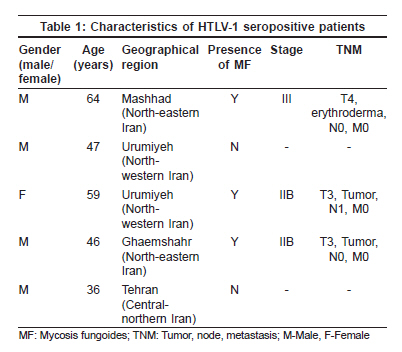
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 363-367 Original Article Comparison of seropositivity of human T lymphotropic virus type 1 in mycosis fungoides patients and normal volunteers: A case-control study and review of literature Seirafi Hassan, Farnaghi Farshad, Firooz Alireza, Mostafa Sana, Talaei-Khoei Mojtaba, Davari Parastoo, Gorouhi Farzam Razi Skin Hospital, Department of Dermatology and Center for Research & Training in Skin Diseases & Leprosy, Medical Sciences/University of Tehran, Tehran Code Number: dv09144 PMID: 19584460 Abstract Background: There have been controversial reports about the possible association between mycosis fungoides (MF), its leukemic variant Sιzary syndrome (SS) and human T lymphotropic virus type 1 (HTLV-1) in different geographical regions. Keywords: Mycosis fungoides, Enzyme-linked immunosorbent assay, Human T-cell lymphotropic virus type 1, Western blot Introduction Mycosis fungoides (MF) is an infrequent, T-cell lymphoma first reported by Alibert [1] in the early 1800s. Primarily, this disease is manifested with plaques, being the typical feature, in skin. Then, it might advance after a variable period of time to cutaneous tumors and invade to visceral sites and lymph nodes [2] Sιzary syndrome (SS) is an erythrodermic, leukemic variant of MF accompanied with presence of circulating tumor cells in blood. [3] The incidence of MF is increasing. In the United States, it has been about 0.4 cases per 100 000 populations, [4] and there has been about 1000 new cases diagnosed every year. [3] Mostly MF/SS is a disorder of middle-aged adults[5] and male to female ratio is 2.2 : 1. [4] The certain etiology of MF is unknown and has remained controversial. A range of theories point the finger at infectious agents, oncogenes, cytokines or occupational or environmental exposures. [1] Several viruses have been implicated in the pathogenesis of MF/SS. There is probable convincing evidence that human T-cell lymphotrophic virus-1 (HTLV-1) is associated with MF; [6] however, these observations are still a matter of debate. One of the prominent supporting evidence of association between MF and HTLV-1 has shown HTLV-1 DNA sequences in peripheral blood mononuclear cells and skin lesions of some patients with MF. [7],[8] On the other hand, some studies have claimed no role for HTLV-1 in pathogenesis of MF. [9] HTLV-1 was first isolated and typified in 1980. This retrovirus provokes the proliferation of CD4+ T-cells and transforms them into tumor cells, mainly resulting in adult T-cell leukemia. HTLV-1 is spread globally with some high endemic foci in southern Japan, intertropical Africa, the Caribbean, certain areas of southern America, Melanesia and Middle East. [10] Mashhad, a city in North-eastern Iran, is suspected for being the ′epicenter′ of HTLV-1 in Middle East and probably in Asia. It was found that the HTLV-1 infection in Israel is limited to Jews originating from Iran, mostly from Mashhad. [11] Therefore, controversy of association of MF and HTLV-1 from one side and endemic status of MF in Iran from another side, persuaded us to retrospectively investigate on the rate of HTLV-1 infection in Iranian MF patients and compare it with its normal rate in Iranian population in a case-control study. Methods Patients The country was divided into five geographical areas: North-eastern, South-eastern, North-western, South-western and central parts. Any occupation in the 10-year period prior to the first clinical evidence of MF was recorded. Personal and family history of malignancies was also investigated. Diagnosis and staging of MF World Health Organization (WHO) classification [12] and International Society for Cutaneous Lymphomas (ISCL) [13] tumor node metastasis (TNM) staging were used for this study. Diagnostic laboratory methods for HTLV-1 Statistical analysis of data Results Mean ages of MF and healthy groups were 44.7 ± 16.2 and 42.3 ± 17.1, respectively ( P > 0.05) Male-female ratios of MF and healthy groups were 1.20 and 1.15, respectively ( P > 0.05). Male subjects had a peak at sixth decade of age and females at fourth decade in both groups. Thirty five (41.6%) male MF patients were farmer and 63 (95.5%) female MF patients were housekeeper. Five (3.3%) MF patients had a history of malignancy: Two with Kaposi′s sarcoma and one for Hodgkin′s lymphoma, non-Hodgkins lymphoma and leukemia each. Healthy controls did not have a history of malignancy at all except one with small cell carcinoma. The majority of patients with MF (113 [75.3%]) were in the initial stages (IA, IB, IIA); however, the three seropositive patients were in advanced age and stage of the disease. Two patients were in stage IIB (tumor stage) and one in stage III (erythroderma). Antibodies to HTLV-1 were found in the sera of only 3 (2.0%) patients with MF by ELISA, which confirmed by blotting and only 2 (1.3%) control volunteers had these antibodies [[Table - 1], P > 0.05]. Discussion Mycosis fungoides is considered to be a sporadic disease. Persistent antigenic stimulation has been proposed as an initial event in MF, but the nature of the involved antigen(s) is unknown. [14] A pathogenic role for a variant or defective retrovirus has been suggested but remains unclear. The etiological role of HTLV-1 in adult T-cell leukemia lymphoma has been firmly established. Poeiz et al . were the first to isolate HTLV-1 from a patient thought to have MF but later diagnosed as having adult T-cell lymphoma leukemia. [15] Later, Pancake and Zucker-Franklin [16] demonstrated HTLVI-1 tax sequences in cell lysates from peripheral blood mononuclear cells of 10 patients with MF. In another study, they showed both Pol and Tax sequences in 46 of 50 MF patients. [17] A study conducted in Germany suggested that HTLV-1 plays a cofactor role in some MF or SS patients. [18] Zucker-Franklin et al . suggested that the prevalence of infection with HTLV-1, particularly when efforts are made to detect Tax sequences may be considerably higher than is currently believed. Although most patients with the cutaneous T-cell lymphoma, MF, are seronegative for HTLV-1, when tested by assays that measure only antibodies to the viral structural proteins, the majority of such patients harbor HTLV-l-related Pol and Tax proviral sequences that encode proteins not included in routinely used serologic tests. Tax mRNA has also been detected in their peripheral blood mononuclear cells. [19] In contrast to these supportive studies, some investigations showed no role for HTLV-1 in MF pathogenesis. [20] Fuhihara et al. proposed that MF and SS were not associated with any of the known prototypic human retroviruses. [21] A study in Pakistan concluded that the prevalence of MF in Pakistan population is comparable to the Western data, and that Epstein-Barr virus (EBV) and not HTLV-1 association to MF cases was higher than in Western studies. [22] A large study conducted by Bzarachi et al. on 127 patients (85 MF, 28 SS, 5 Sιzary cell leukemia, 4 lymphomatoid papulosis and 5 unspecified cutaneous T-cell lymphomas) originating from Europe (France, Spain, UK, Portugal) or from USA (California) for the presence of HTLV-1 infection markers obviously point toward that MF and SS were not associated with HTLV-1 infection. [9] In lymphoproliferative disorders, except adult T-cell leukemia (ATL), [23] the seronegativity for HTLV-1 is common. However, more sensitive methods such as ELISA have recently enabled to show seropositivity for HTLV-1 up to 30% in various leukemia/lymphoma patients including MF. [6],[24] In a study from Japan, 128 DNA specimens of fresh skin lesion have been examined. They showed that none had serum HTLV-1 antibodies to clarify the relationship between HTLV-1 and cutaneous T-cell lymphoma (CTCL) in Japan. [25] To this end, peripheral blood mononuclear cells from HTLV-1 seronegative Tax-only-positive MF patients or from healthy Tax-only-positive blood donors were injected into adult rabbits, an established animal model for HTLV-1 infection. The peripheral blood mononuclear cells of all injected rabbits became Tax sequence positive. These observations proposed that HTLV-1 Tax can be transmitted by Tax-only-positive mononuclear cells. [26] There are several possible explanations for these contradictory results: (i) Technical problems such as contamination of PCR reactions can easily occur especially in PCR studies; (ii) Many positive bands can be detected if the stringency of PCR is low, [25] unless the complete sequencings for the PCR products are done; [27] (iii) Differences in the selections of patients; (iv) The involvement of the retrovirus related to but different from HTLV-1, deleted forms of HTLV-1genome might exist in the genomic DNA of CTCL patients. [28] Lastly, in the positive studies most of the HTLV-1 DNAs were proved not in the fresh specimen but in the cultured cells including non T-cell lines. [28] During the cultivating procedure, not only colony expansions but also modifications of the culturing cells can occur. Thus the DNA derived from these cell lines does not exactly reflect conditions in the original CTCL. Furthermore, HTLV-1 sequences have been detected even in the squamous cell carcinomas of the skin [29] proposing that an opportunistic or a coincidental infection of HTLV-1 should be considered. In the present study, after conducting an antibody ELISA test of the 150 MF patients, only 3 (2%) positive responses have been reported and 2 (1.3%) individuals in the control group had antibodies to HTLV-1. Analysis confirmed the lack of any statistically significant association between MF and HTLV-1, and in conclusion evidence for a primary etiologic role of this virus in MF is lacking. A wide range of geographical distribution have been reported by both patients and control subjects, two seropositive patients with MF were from east-northern Iran: One from Mashhad and the other from QaemShahr. No obvious or significant differences were seen with regard to endemic area Mashhad for HTLV-1. In contrast, a study had described a high overall risk of HTLV-1 infections in Israelis originating from the city of Mashhad. [30] The prevalence of HTLV-1 infection in Mashhad is estimated to be 2-3% in the whole population and 0.7% in blood donors. [31],[32] It has been shown that some HLA alleles, which are more common in Mashhad residents, can increase the risk of occurrence and severity of HTLV-1. [33] A more recent study from Germany in over 82 patients with primary cutaneous lymphoma, has observed an elevated risk for the development of a secondary lymphoproliferative disorder even without previous chemotherapy. [34] In studies of this type, it is always important to guard against selection bias (epidemiological trends) in the population studied. The major limitation of this study has been its case-control design. It is hardly concluded a definite fact out of a case-control study design. Taken together, our study shows that there is no significant clustering of other malignancy in patients affected with MF. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09118t1.jpg] |
| |||||||||

{kind=link}