 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
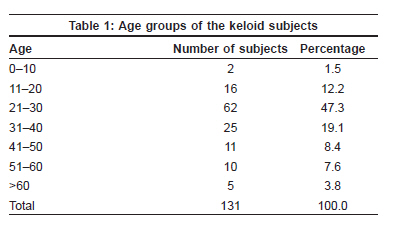
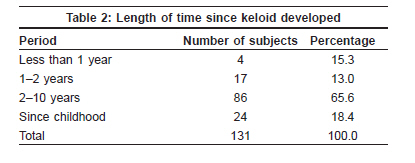
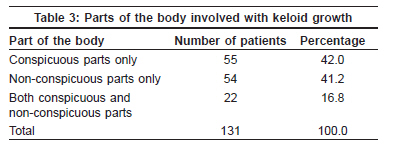
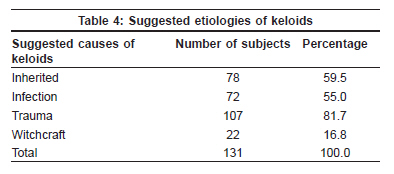
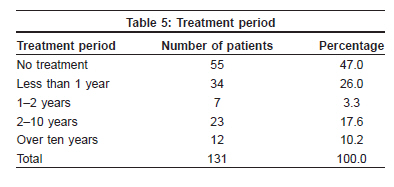
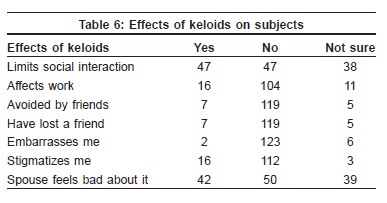
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 368-372 Original Article Keloids: Assessment of effects and psychosocial- impacts on subjects in a black African population Olaitan PB Department of Surgery, Lautech Teaching Hospital, Osogbo, Osun State Code Number: dv09145 PMID: 19584461 Abstract Background: Keloids are vexatious swelling on the skin or the conjuctiva. The effects and impacts of these lesions have not been assessed in a keloid endemic environment like Nigeria. Keywords: Keloid, Impact, Psychosocial, Black Introduction Despite their common occurrence, keloid remains one of the most challenging dermatologic conditions to successfully treat and may have significant psychosocial impact on the patient. Keloid and hypertrophic scars have affected patients and frustrated physicians for centuries. [1] More than a cosmetic nuisance, they are often symptomatic and can have a significant psychosocial burden for the patient. They might turn out as an esthetically unacceptable complication of wound healing and some scars might even cause anatomic dysfunction. [2] Worse still is the fact that the swellings may be multiple, located in a site that cannot be masked and constitute an embarrassment to the patients from friends and other people. While typically only impinging on cosmesis, large or recurrent keloids may require therapeutic intervention. [3] In such instances, treatment may be impossible or at best difficult. Patients may therefore be psychologically affected. Scars can have many significant functional, cosmetic and psychological sequelae. [4] Perception and psychosocial impacts of these benign but disturbing tumors is studied and presented in this paper. Keloids is said to be endemic in black Africa. It is therefore important to assess the perception of the subjects with these complications of wound healing to keloid problems among the population. The objectives of this study was therefore to assess the perception of the subjects with keloids, the psychosocial impacts and effects as well as how patients with keloids cope with them in a black African community where keloids have been found to be very common. Methods A prospective study of patients who presented to the surgical outpatient clinic of the Plastic Surgery Clinic of the Lautech Teaching Hospital, Osogbo, with keloid swellings was carried out. This study took place between January 2005 and June 2008. Questionnaires were distributed among the patient who consented to take part in the study following ethical approval. None of the patients who presented with keloids and consented to participate in the study was excluded from the study. The questionnaires were designed to find out the perception of the keloid patients to keloids and find out the psychosocial impact of the pathology on the affected patients. Information required from the patients included their bio-data, length of period they have carried the keloid, symptoms of keloids, site of keloids - whether or not it is located at an obscure or visible site, whether or not the symptoms affect their daily routine, etc. The data were analyzed using SPSS Version 10.Results One hundred and thirty one keloid cases were involved in this study. They were all Yorubas from the South Western Nigeria. There were 61 males and 70 females. Their age ranges between 14 and 66 years with an average of 31.74 ± 34 years. One hundred and ten (80.2%) of them had at least secondary education while only 10 (7.6%) never had any form of education. The age groups of the subjects are as shown in [Table - 1] with the age group of 21-30 being most (47.3%) affected with keloids followed by age group of 31-40 (19.1%). One hundred and ten (83.97%) of the patients had had the swellings on the skin for more than two years, while 24 (18.32%) had swellings since childhood [Table - 2]. Fifty five (42.0%) of the patients had keloids in conspicuous parts of the body alone i.e. hand, forearm, head and neck, 54 (41.2%) on non-conspicuous parts, while 22 (16.8%) had the swelling on both conspicuous and non-conspicuous parts of the body [Table - 3]. Sixty one (46.6%) of the patients had family history of keloids while 64 (48.9%) had no positive family history of keloids and 6(6.4%) were not sure of anybody in the family with keloids. Suggested possible causes of keloids by the respondents include heredity, 78 (59.5%); infection, 72 (55.0%); trauma, 107 (81.7%) and witch-craft, 22(16.8%) [Table - 4]. One hundred and five (80.2%) of the respondents correctly stated that keloid is not contagious while 9 (6.9%) think it can spread from one person to another and 14 (10.7%) were not sure. Although the patients had carried lesions for many years [Table - 2], only 39 (28.9%) of them had been to a doctor before presentation, while 92 (70.3%) never presented to a doctor before the presentation at our clinic. While 34 (26.0%) of the patients had been on treatment for keloids for less than one year, 42 (32.06%) of them had been treated for a period of one year to over ten years and 55 (47.0%) had never had any treatment for their keloid lesions [Table - 5]. Of the 76 (58.0%) patients who were on treatment, only 25 (19.1%) had received orthodox treatment. Fifteen (14.5%) of the patients were on the topical application of the locally made shea butter (ori) ointment, the remaining 36(27.5%) were on snake fat (ora ere). When asked about the impact of keloids on the patients, the number of patients who believed that keloid swelling limit their social interaction was 47 (35.9%) which was equal to the number who believed that keloids do not limit their social interaction [Table - 6]. One hundred and four (79.4%) believe that keloids do not have negative effects on their jobs while 16 (12.2%) of them claim that keloids affect their work. Of the 16 who claimed that keloids affect their works, 7 of the patient were females while 9 are males. No significant difference was, however, observed between the two sexes when comparing the effects on their jobs. Among the patients whose works were affected by keloids, 4 (25.0%) claim this happened when keloids get infected and sting, 12 (75.0%) of them stopped work because they felt psychologically troubled by keloids. Significant number (119 or 90.8%) of the patients felt that friends freely relate with them in spite of the keloid swelling, while 7 (5.3%) of the patients claimed that they observe that their friends avoid them. One hundred and twenty three (93.9%) of the patients did not feel embarrassment by keloids while only 2 (1.5%) patients felt embarrassment by the presence of keloids. When considering stigma, 64 (48.9%) of the patients feel stigmatized by keloids while 55 (42.0%) of the patients do not feel stigmatized. Twenty eight (56.0%) of the patients who felt stigmatized had lesions in conspicuous parts while 24 (46.2%) had lesions in non-conspicuous parts. On the other hand, 26 (50.0%) of those who had keloid lesions in hidden parts of the body did not feel stigmatized compared with 21 (42.0) patients who had keloids in conspicuous parts and did not feel stigmatized. These differences were, however, not significant ( P < 0.001). Although more females (39 or 59.1%) felt stigmatized by the presence of keloids than males (25 or 45.5%), this was not statistically significant. Expectedly, of the 24 patients who felt keloids had affected their relationship with others, 17(70.8%) had keloids in conspicuous parts of the body, while only 3 (12.5%) had them in non-conspicuous parts and 4 (16.7%) had keloids in both conspicuous and non-conspicuous parts. There was a statistically significant difference among those who had lesions on conspicuous parts and feel their relationship was affected and those who had them in non-conspicuous parts with the same feeling. When asked how the patient felt with keloids, 74 (56.5%) felt keloids were parts of their bodies and cope very well with it, 11 (8.4%) always feel ashamed and hide the keloids, 2 (1.5%) patients took rest when they had pain or itching while 9 (6.9%) of the patients found it difficult to cope with keloids. Suggested methods of preventing keloids by the respondents included avoiding wounds and accidents, 70 (53.4%), early immunization and avoiding scratching suggested by one patient each, while 36 (27.5%) did not know how to prevent keloids. Discussion For centuries, keloids have been an enigma. [5] Keloid management can be difficult and frustrating, (both to the patient and the attending physician) and mechanisms underlying keloid formation are only partially understood. [6] In fact, keloids and hypertrophic scars have affected patients and frustrated physicians for centuries. [1] Although people of all ages suffer from these conditions, the patients are often young and otherwise healthy, and become burdened with an activity limiting lesion or psychosocial stresses associated with a perceived esthetic defect. [5] The average age of the patients in this series is 31.74 ± 34 years, showing keloids as a rather young age medical problem. Majority of the patients correctly identified the possible etiologies of keloid lesions in this study showing a good knowledge of etiology of the problem. It could be suggested that this is because the pathology is common in this environment. The patients carried lesions for several years with 86 (65.6%) of them having carried the lesions for 2-10 years, while 24 (18.4%) of them have lesions since childhood [Table - 1]. The lesions had been present on respondents for an average of 4.6 ± 2.6 years. This shows the chronic nature of these lesions and indeed a number of these patients had sought one form of treatment or another for a long time with no or little improvement. It has been observed that keloids remain one of the most challenging dermatologic conditions to successfully treat and may have significant psychosocial impact for the patient. [7] Only 16 (12.2%) of the patients in this study complained that keloids had effect on their works, while 104 (79.4%) claimed that keloids have no effect on their works. This suggests that keloids do not affect daily chores of a significant number of keloid patients in this study. However, those who claimed that keloids affected their jobs also claimed that this happened when they had pain or when the keloid was infected and gave offensive odor. Keloids as a complication of wound healing have been observed to be esthetically unacceptable to the patient. [2],[8],[9],[10] It has also been observed that patients′ dissatisfaction and psychological issues may arise from scarring. [11],[12],[13] Although people of all ages suffer from these conditions, the patients are often young and otherwise healthy, and become burdened with an activity limiting lesion or psychosocial stresses associated with a perceived esthetic defect as observed by Meier and Nanney, [14] and severe negative impacts on the quality of life of patients with keloids have also been reported. [15] Forty seven (35.9%) of the patients in this study claimed that keloid lesions limit their social interaction while an equal number of patients interact freely without any limitation. Although most, 123 (03.9%) of the patients were not embarrassed by the presence of keloids, more patients (64 or 52.5%) consider keloids as creating stigma, while 55 (45.1%) of the patients did not think keloids create stigma. It could be observed from this study that most of the respondents were aware of the non-contagious nature of keloid lesion and thus be able to educate others on keloids. Of the 131 patients, only 76 (58.0%) were on one form of treatment or the other; others not having any treatment at all. The patients possibly did not consider keloids as a significant health problem to warrant treatment especially since it was not a painful problem. Twelve (15.8%) of the respondents had been on treatment for more than 10 years revealing the chronic nature of this pathology as well as the economic implication on the patients. Sixteen of the patients claimed that keloids affect their works; 4 due to infected keloids with emanating bad odor and the others for psychological problems associated with keloids. Robles and Berg [7] have described keloids as more than a cosmetic nuisance and that they are often symptomatic and can have a significant psychosocial burden for the patient. The problem of scarring represents a large area of an unmet medical need, since people with abnormal skin scarring may face physical and psychological consequences that may be associated with substantial emotional and financial costs. [16] It is to be concluded that the knowledge of etiology and prevention of keloids is high in a keloid-endemic environment like Nigeria. Patients with these lesions possibly do not consider lesions as a great problem and rarely present to physicians. They also do not have significant social problems or problems with their daily chores. We can therefore conclude that unlike in white population with serious negative impacts of keloids among the keloid patients as noted by Bock et al ., [15] most keloid patients in a black African community are still able to cope considerably better than their counterparts in areas of low incidence of these lesions. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09119t6.jpg] [dv09119t1.jpg] [dv09119t5.jpg] [dv09119t4.jpg] [dv09119t2.jpg] [dv09119t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}