 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
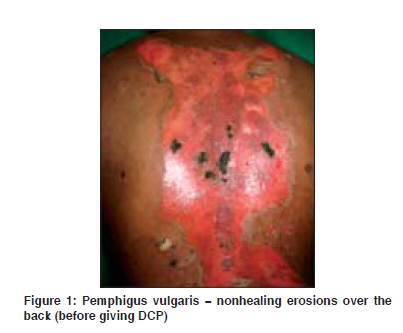
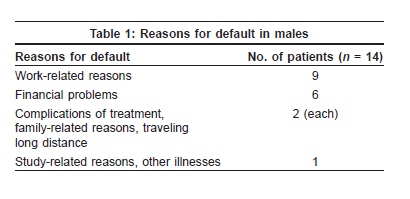
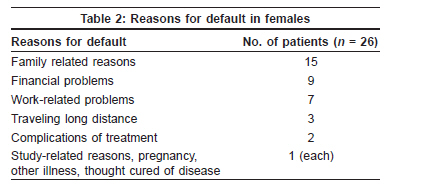
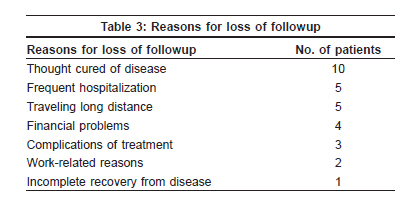
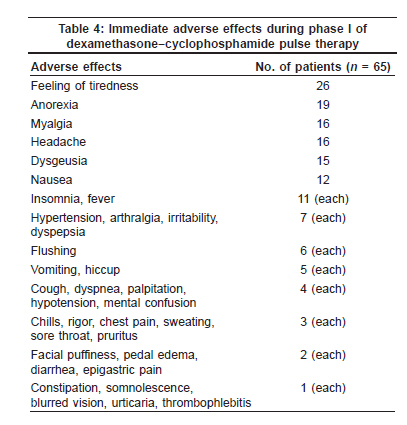
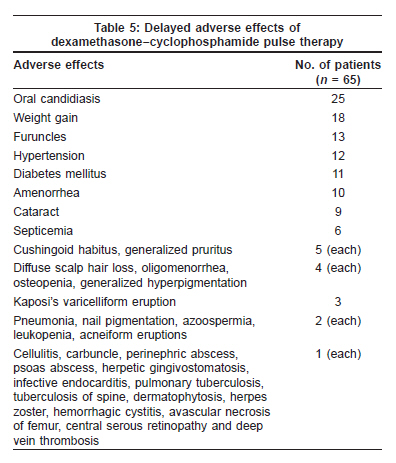
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 373-378 Original Article Outcome of dexamethasone-cyclophosphamide pulse therapy in pemphigus: A case series Kandan Sakthi, Thappa DevinderMohan Departments of Dermatology and Sexually Transmitted Diseases (STD), Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006 Code Number: dv09146 PMID: 19584462 Abstract Background: Pemphigus disorders are a group of serious and potentially life-threatening diseases affecting skin and/or mucus membranes. Dexamethasone−cyclophosphamide pulse (DCP) therapy has shown promising results in the management of these diseases.Aims: The objective of the study was to assess the outcome of DCP therapy in pemphigus. Methods: Pemphigus patients who had been treated with DCP therapy from 2001 to 2008 were prospectively and retrospectively analyzed. Results: A total of 65 pemphigus patients were enrolled. Male to female ratio was 1 : 1.82. Mean age of patients was 44.65 ± 11.85 years with a range of 14 to 73 years. Thirty two patients completed phase I, of which 28 (9 in phase II, 7 in phase III and 12 in phase III) were maintaining remission and four patients relapsed. Relapse was observed only in patients who discontinued or took irregular treatment. Six patients were declared cured of disease. Five patients died during phase I. Dexamethasone−cyclophosphamide pulse therapy is not absolutely free from adverse effects. Most of the immediate side effects were expected, tolerable and did not pose any problem in continuing treatment. There was a slight increased incidence of weight gain, hypertension, diabetes mellitus, cataract and Cushingoid habitus, since most of our patients also received additional daily oral steroids. Also, there was a high incidence of secondary pyogenic infections of skin lesions and oral candidiasis during phase I. Staphylococcus aureus was the commonest bacteria isolated from the pus of skin lesions. Most of the alterations in laboratory parameters were transitory or correctable, and did not pose a problem in continuing therapy. Conclusions: DCP therapy was found to be effective in inducing and maintaining remission in pemphigus, provided the patients receive regular and complete treatment. Keywords: Pulse therapy, Dexamethasone, Cyclophosphamide, Pemphigus Introduction Pemphigus disorders are a group of serious and potentially life-threatening disorders characterized by blisters in the skin and/or mucus membranes.[1] Dexamethasone−cyclophosphamide pulse (DCP) therapy designed by Pasricha et al. at All India Institute of Medical Sciences (AIIMS), New Delhi, has revolutionized the management of pemphigus since its introduction in 1986. [2] If properly used, DCP therapy has the potential to effect lifelong recovery from these diseases. [3] Apart from pemphigus, DCP therapy was also found to be effective in pemphigoid disorders, systemic sclerosis, SLE, etc. [4] Here, we report the outcome of DCP therapy in 65 patients with pemphigus.Methods We prospectively analyzed the patients with pemphigus treated with DCP therapy from August 2006 to June 2008 in the Department of Dermatology and STD, at our institute. Also, retrospective analysis of patients who had been treated with DCP therapy from August 2001 to July 2006 was done. The diagnosis in these cases was based on clinical features, Tzanck smear, histopathology of the skin/mucus membrane lesions and direct immunofluorescence test. One hundred and twenty milligrams of dexamethasone dissolved in 200 ml of 5% dextrose (instead of 100 mg of dexamethasone in 500 ml of 5% dextrose as in the original regimen designed by Pasricha et al. [5] was administered as a slow intravenous infusion over two hours for three consecutive days, and 500 mg of cyclophosphamide was added in the same drip on the second day. This constituted one DCP. Such DCPs were repeated at exactly 28 days interval counted from the first day of the previous DCP. In between DCPs, patient received 50 mg of cyclophosphamide orally per day. During the first few months (phase I), the patient may continue to develop clinical lesions in between DCPs. To achieve quick remission (absence of fresh lesions and disappearance of the existing lesions), [6] 40-60 mg of prednisolone per day orally or additional dexamethasone pulses were given in addition. Prednisolone was tapered stepwise during the subsequent DCPs. After the skin and mucosal lesions subsided completely and the additional medications were withdrawn, the patient was shifted to phase II. In phase II, nine more DCPs were administered along with 50 mg cyclophosphamide orally per day. In phase III, DCPs were stopped; only 50 mg of oral cyclophosphamide was given daily for 9 months. In phase IV, all treatments were stopped, and patients were followed up as long as possible to look for any tendency to relapse. If a patient did not develop a relapse for two years after complete withdrawal of treatment, he was declared to be cured of disease. Data regarding the age, gender, age of onset of disease, clinical details about the disease, previous treatment details, phases of therapy, remission, relapse, cure, default and reasons for default, death and causes of death and adverse effects of therapy were recorded. The severity of skin involvement was categorized as mild, with less than 20 blisters, moderate with 20-40 blisters and severe with more than 40 blisters. Mucosal involvement was categorized as mild, with 1-5 lesions, moderate with 5-10 lesions and severe with more than 10 lesions or extensive erosions.[7] Laboratory investigations such as urine analysis, stool analysis, hemoglobin, total and differential leukocyte counts, platelet counts, blood sugar, blood urea, serum creatinine, serum electrolytes and liver function tests were done before each pulse. Any alterations from the standard normal values were noted. Bacterial culture and sensitivity were done from infected skin lesions. Ethical clearance was obtained from the Institute Ethical Committee for both prospective and retrospective cases. Results Of the 65 pemphigus patients enrolled for DCP therapy, 42 (64.6%) were females and 23 (35.4%) were males. Male to female ratio was 1 : 1.82. Mean age of patients was 44.65 ± 11.85 years with a range of 14- 73 years. Majority (40) of them belonged to age group of 40-59 years, followed by 20-39 years (17), 60 years and above (6) and less than 20 years (2). Mean age of onset of disease was 41.91 ± 12.15 years with a range of 13- 72 years. Disease profile Amongst the 65 patients, 64 patients had skin involvement. Amongst these 64 patients, 42 (65.62%) patients had severe skin involvement, 16 (25%) moderate skin involvement, and 6 (9.38%) mild skin involvement. Among the 49 pemphigus vulgaris patients, 47 had oral involvement. Of the 47 patients, 27 (57.45%) of them had severe disease, 14 (29.79%) had moderate disease and 6 (12.76%) had mild disease. The one patient with paraneoplastic pemphigus had severe oral mucosal disease. Previous treatment Duration of the disease prior to initiation of DCP therapy Phases of DCP received by patients Phase I: Among the 33 patients, 14 patients are receiving DCPs, 8 patients discontinued therapy, 6 patients were shifted to other forms of treatment for various reasons and 5 patients expired. Interestingly, among the 8 patients who discontinued treatment after receiving some pulses in phase I, three were in remission (disease-free period 5 years in one patient and 6 years in 2 patients) until now without any treatment. Phase II: Twelve patients reached phase II, of which 6 patients are continuing therapy and were in remission, the remaining 6 patients discontinued therapy. Among the six patients who discontinued treatment, 3 came back with relapse and 3 were in remission (one patient for 9 months, and two patients for 4 and 5 years, respectively) without any treatment. Phase III: Seven patients reached phase III and all were in remission. Phase IV: Thirteen patients reached phase IV, of which 12 are in remission and one patient relapsed. Among the 12 patients who are in remission, six patients completed two years in phase IV and were declared cured of disease. A total of 32 patients completed phase I and were in phase II, phase III or phase IV [Figure - 1] and [Figure - 2]. Mean number of pulses required in phase I was 9.53 ± 3.52 with a minimum of 5 pulses (2 cases) and maximum of 20 pulses (1 case). Majority (22) of them needed 6−10 pulses to achieve remission. Fifty eight (89.2%) patients also received daily oral prednisolone in between DCPs in phase I. Seven (10.8%) patients did not receive oral steroids in between DCPs. Ten patients also received additional dexamethasone pulses (ADP) in between DCPs in phase I at two weeks interval. Eight patients received only one ADP and two patients received two ADPs. Five (7.7%) patients died while on therapy. The causes of death were septicemia in two cases, septicemic shock and adult respiratory distress syndrome (1), pre-renal failure and cardiorespiratory arrest (1) and sudden cardiac arrest (1). Forty (14 males and 26 females) patients were irregular in receiving pulses due to various reasons. Most of the patients had more than one reason for irregular treatment [Table - 1] and [Table - 2]. Fourteen patients lost to followup during treatment, eight patients in phase I and 6 patients in phase II [Table - 3]. The adverse effects that were observed during infusion, pulse days and within a week of starting each pulse were considered as immediate adverse effects. Those side effects that occurred later than 7 days after each pulse, in between various pulses (during phase I and II) or later on during phase III and IV were taken as delayed adverse effects. The immediate adverse effects that were observed during phase I are tabulated in [Table - 4]. In most of the patients, the effects reduced in severity and frequency during phase II. The delayed adverse effects observed during all four phases are tabulated in [Table - 5]. Leukocytosis was observed in 15 patients, followed by hyperglycemia (10), hypocalcemia and eosinophilia in 6 patients each, elevated serum alkaline phosphatase (5), anemia (4), leukopenia, elevated aspartate aminotransferase (AST) and alanine aminotransferase (ALT) in two patients each, hypernatremia, hyponatremia and hypokalemia in one patient each. All the changes were transient or correctable and did not pose any contraindication for continuing therapy. Pus culture reports were available only in 44 patients. In five patients, more than one bacterium were isolated. Staphylococcus aureus was isolated in 24 cases, followed by methicillin resistant S. aureus in 10 cases. All the 24 S. aureus isolates were sensitive to vancomycin and oxacillin, 9 to ciprofloxacin, 8 to tetracycline, 5 to gentamycin, 4 to erythromycin, 4 to penicillin, 3 to ceftriaxone and 2 to ceftazidime. All the MRSA isolates were sensitive to vancomycin, and two to ciprofloxacin, and resistant to all other drugs. Discussion Pulse therapy has revolutionized the treatment of pemphigus from mere control of disease to probable cure. [2] The results of our study indicate high degree of positive outcome in terms of effectiveness of DCP therapy. We were able to maintain remission in 87.5% of cases who completed phase I. Sacchidanand et al. [6] reported remission in 41 (82%) patients in their study on 50 patients with autoimmune bullous disease treated with DCP therapy. Pasricha et al. [3] achieved remission in all the 103 pemphigus patients treated with DCP therapy. We were able to induce remission in almost all patients in whom the disease was not controlled by varying doses of daily oral or parenteral steroids given from other centers. Majority of the patients (22) needed 6-10 pulses to achieve remission in phase I. However, few patients needed up to 16-20 pulses to achieve clinical remission. Pasricha et al. [8] also made similar observation where nearly 50% of patients achieved remission with 6 or less DCPs; however, 11% patients took more than two years to achieve complete clinical remission. However, in a recent study by Pasricha et al. , [3] the addition of betamethasone in between DCPs helped to shorten the duration of phase I to 3-4 months in most of the patients. Relapse, defined as recurrence of the disease after having completely recovered from the disease, is mostly observed in patients who receive either incomplete or irregular treatment. [5],[8] The treatment administered during phases II and III is necessary for ultimate clinical cure. [5] We observed relapse only in 4 (12.5%) out of the 32 patients who completed phase I. Among these 4 patients, three had discontinued therapy during phase II and one patient relapsed during phase IV. Also, all these four patients were very irregular in receiving DCPs. Recently Pasricha et al. [3] reported a low-relapse rate of 7.7%, where majority of the patients completed the regimen strictly according to the prescribed schedule. Our finding is in accordance with other studies where the relapse rates were higher in patients who received irregular and incomplete treatment. [5],[8] Most of the relapses in pemphigus patients treated with DCP therapy are known to occur during the first two years of posttreatment followup period only. Therefore, if patients with pemphigus do not develop a relapse for two years after complete withdrawal of all treatments, they can be considered to have been cured. [9] On this basis, six pemphigus patients in our study declared to have been cured of the disease. Mahajan et al. [10] observed a high rate (58%) of drop out in pemphigus patients treated with DCP therapy. The probable reasons were frequent hospitalization, higher cost of therapy, complacency of cure once lesions healed and traveling longer distance to treatment center. In our study, the most frequent reasons for defaulting and irregularity in case of males were mainly work-related followed by financial problems, whereas in case of females, family reasons and financial problems were mainly responsible for irregular treatment. Most of the patients thought that their disease got cured and further treatment is unnecessary, even though they were repeatedly explained about the nature of disease and treatment. Pasricha et al. [5] in their study on 500 pemphigus patients reported that 19 patients had died due to various causes, which were either preventable with better patient management or unrelated to disease and treatment. In a study by Roy et al. [11] on 37 pemphigus patients treated with DCP therapy, 4 (10.8%) had died. Two patients died of septicemia, one each from peripheral circulatory failure and cardiac arrest. In our study, five (7.7%) patients died during treatment with septicemia as a possible cause in three cases. The death rate in pemphigus patients in our study is comparable to that seen in other study. [11] Pulse therapy is not absolutely free from side effects.[12] The adverse effects of DCP therapy are those of its constituent drugs, i.e. dexamethasone and cyclophosphamide. [13] The adverse effects that were observed by us during infusion or within a week of each pulse such as generalized weakness/feeling of tiredness, myalgia, arthralgia, dysgeusia, hiccup, flushing, palpitation, insomnia and headache have been already reported and they are considered as peculiar adverse effects of pulse therapy. [12],[13] Others such as fever, chills, rigor, sweating, pedal edema and thrombophlebitis can occur with infusion of any drugs. We also observed gastrointestinal adverse effects such as anorexia, nausea, vomiting and dyspepsia. However, almost all patients tolerated these side effects and continued therapy. Generalized weakness or tiredness which lasted for 2-3 days, in some cases up to one week following infusion, was one of the significant complaints by our patients which affected their day to day activities. However, this effect was observed to decrease with subsequent pulses. This effect is considered to be caused by transient adrenocortical suppression due to withdrawal of high doses of dexamethasone used for pulse. However, this can be treated with daily administration of one tablet of 0.5 mg of betamethasone for 3-4 days after the pulse. [9] There is almost no risk of developing diabetes, hypertension, weight gain, Cushingoid habitus, peptic ulceration and osteoporosis with pulse therapy unless the patient receives or had received conventional daily dose of steroids. [5] Secondary pyogenic infections of skin lesions and candidiasis of the mouth during active stage of the disease (phase I) are the most important side effects of DCP therapy observed in earlier studies. [5],[8],[11],[14] We also observed a high incidence of secondary pyogenic infections of skin lesions and oral candidiasis during phase I. Gonadal toxicity of cyclophosphamide is a well-known complication and may manifest as amenorrhea, with or without ovarian failure, infertility and azoospermia. [10] We observed a high incidence of amenorrhea and oligomenorrhea, which is comparable to that observed in other studies. [8],[10] Semen analysis was performed in two patients and both of them had azoospermia. Generalized pigmentation of the skin and nail pigmentation are known to occur in patients treated with cyclophosphamide. [15] We observed generalized pigmentation in four patients and nail pigmentation in two patients. Many earlier studies had indicated that the changes in the laboratory parameters such as leukocyte counts, platelet counts, hemoglobin, blood glucose, electrolyte levels and liver function tests were either insignificant or transient. [8],[11],[16],[17] The laboratory changes observed in our study were transient or correctable and did not pose any contraindication for continuing therapy. To conclude, the results of this study indicate a high degree of positive outcome in terms of effectiveness of DCP therapy in pemphigus. With DCP therapy, it is now possible to induce and maintain remission, and achieve cure, even in patients resistant to other forms of treatment, provided the patients strictly adhere to the prescribed schedule. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09120f1.jpg] [dv09120t2.jpg] [dv09120t5.jpg] [dv09120t4.jpg] [dv09120t1.jpg] [dv09120f2.jpg] [dv09120t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}