 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
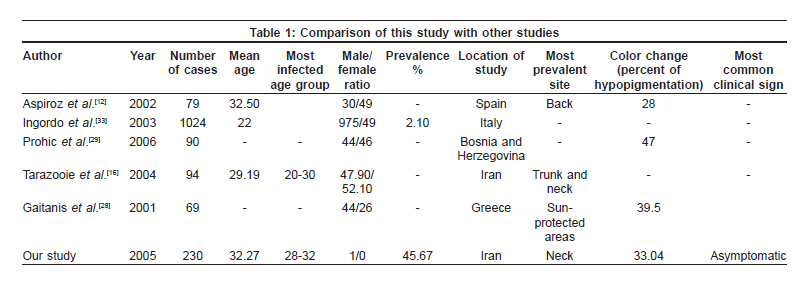
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 379-382 Brief Report Evaluation of pityriasis versicolor in prisoners: A cross-sectional study Salahi-Moghaddam Abdoreza, Davoodian Parivash, Jafari Ali, Nikoo MohammadAli Department of Infectious Disease, Hormozgan University of Medical Sciences, Hormozgan Code Number: dv09147 PMID: 19584463 Abstract Background: Pityriasis versicolor (PV) is a mild but recurrent superficial fungal infection of stratum corneum. Many predisposing factors such as late teen and young adulthood age, tropical and subtropical climate (and to a lesser extent temperate climate), immunosuppression, malnutrition, use of oral contraceptives, hyperhidrosis, poor hygiene and a few other factors have been proposed for this condition.Aim: Regarding these probable and possible risk factors, we felt that jail is a unique population which can be affected by this infection and therefore we decided to evaluate some aspects of this infection in this population. Methods: In this cross-sectional study in male prisoners of Bandarabbas city, 230 prisoners were randomly selected. One hundred and five (45.67%) of them were diagnosed to be infected. They were also evaluated regarding age, duration of being imprisoned, skin color, site of lesion and its pigmentation change and any concomitant clinical manifestation such as pruritis, burning or cebure. Chi-square test or Fisher's exact test was used for data analysis. Results: Mean age of infected population was 31.62 ± 8.67 years while peak incidence of PV was in 28-32 years age group. The most common color change was hypopigmentation. No case of PV hyperpigmentation was seen. We could not also observe any association between skin color and duration of being imprisoned with the frequency of infection. Conclusion: There seems to be no difference between pattern of infection in the general population and prisoners' population in the aspects evaluated. Keywords: Pityriasis versicolor, Prisoners, Epidemiology Introduction Pityriasis versicolor (PV) also called tinea versicolor is a mild but recurrent superficial fungal infection of stratum corneum. This infection presents most commonly as pigmentation changes in the skin but also can be accompanied with cebure or pruritis. [1],[2] Genus Malassezia has a definitive causal role in the pathogenesis of PV. [3] This fungus is part of normal skin flora but is also implicated probably in the pathogenesis of many other conditions such as atopic dermatitis, seborrhoeic dermatitis, reticulate papillomatosis, pityriasis capitis and psoriasis as well as systemic infections. [4],[5],[6],[7],[8] Many species exist in this genus while the most common isolated form from skin lesions is Malassezia globosa . [9],[10],[11],[12],[13],[14],[15],[16] Many predisposing factors have been proposed for this disease such as late teen and young adulthood age, [17],[18],[19],[20],[21] tropical and subtropical climate (and to a lesser extent temperate climate), immunosuppression, [18] use of oral contraceptives, [22] hyperhidrosis, [23] malnutrition, [24] poor hygiene [25],[26],[27] and a few other conditions. From mentioned factors only the first three have been proved to be definitively predisposing and role of others are still under question. Regarding these probable and possible risk factors, we thought that jail is a unique population affected by this infectious agent, therefore, we decided to evaluate some aspects of this infection (PV) in them. Methods We conducted this descriptive cross-sectional study in male prisoners of Bandarabbas city - with a tropical or subtropical climate - in the year 2006. Our sample size was 230 persons with a mean age of 32.27 ± 8.26 years that were randomly selected between 1489 persons in the jail of Bandarabbas city. All selected prisoners were examined and specimens for direct microscopic examination were taken from the site of lesion. In the absence of such lesion, specimens were taken from back of the neck of these prisoners by scraping the site with a scalpel. Also a questionnaire was filled by selected prisoners and examiner including age, duration of staying in jail, skin color, site of lesion and its pigmentation change and any concomitant clinical manifestation such as pruritis, burning or cebure. The study protocol was approved by research ethics committee of Hormozgan University of Medical Sciences and every patient gave informed consent before enrollment in the study. All specimens were delivered to mycology and parasitology laboratory of medical university of Bandarabbas. Smears were prepared with 10% KOH and methylene blue for direct microscopic examination with x10 and x40 magnification power. Infection was assessed by observing morphological features of Malassezia (budding cells and/or hyphae) by researcher - a sixth year medical student. All positive results and 10% of negative results were also examined by one of attendings of department and a mycologist in the laboratory to evaluate the accuracy of researcher′s microscopic examination. Numerical variables were presented as mean ± SD and categorized variables were summarized by absolute frequencies and percentages. Categorical variables were compared using Chi-square test or Fisher′s exact test if required. For the statistical analysis, the statistical software SPSS version 13.0 for Windows (SPSS Inc., Chicago, IL) was used. All P values were two-tailed with statistical significance defined by P ≤ 0.05. Results From 1489 male prisoners, a total of 230 persons were randomly selected with a mean duration of staying in jail of 5 ± 1.8 months. In this population, 56 (24.34%) persons had bright skin color and 174 (75.65%) persons had dark skin color. Finally 105 (45.67%) of them were infected and 125 (54.33%) were not infected. Mean age of infected population was 31.62 ± 8.67 years while peak incidence of PV was in 28-32 years age group. The most common color change was hypopigmentation. No case of PV with hyperpigmentation was seen. Neck (35.2%) was the commonest site of lesion followed by chest (14.3%) and back (9.5%). Other sites were involved in 21.9% of the cases. Itch (27.6%) and cebure (6.7%) were the commonest signs. 65.7% of patients were asymptomatic. On comparing dark and bright skin prisoners, we could not find any significant difference in prevalence of infection between these two groups. Also, we could not observe any association between duration of staying in jail and frequency of infection ( P > 0.05). Discussion The prevalence of PV in this study was 45.67%. Hypopigmentation was the most frequent color change and absence of any concomitant symptom or sign was the most common associated clinical manifestation. Back was the most common site of involvement and the peak incidence of PV was in 28-32 year age group. Hypopigmentation as the most common color change and lack of concomitant sign and symptom as the most common associated clinical manifestation has also been implicated in many other studies. [12],[28],[29] We also could not find any association between color of skin and frequency of infection. The sites which are commonly involved in our study are the same as many other studies [11],[13],[16],[19],[21] and our study does not show any tendency for involvement of a special site in our population. Prevalence of PV greatly depends on climate with prevalence as low as 0.5% in temperate climate through prevalence as high as about 50% in tropical and subtropical areas. [9],[16],[23],[29] As Bandarabbas is a city with tropical or subtropical climate, the prevalence should be near upper range in the general population in this city but to determine the exact prevalence in general population, there is no data available, so we cannot definitively compare frequency of infection between prisoners and general population. The age category most commonly reported in the literature was about 20-30 years which seems to agree with our study and it seems that there is no age preponderance in this population in comparison with other studies. [16],[29],[30],[31],[32] As we could not find any statistically meaningful association between duration of being imprisoned and frequency of infection; it seems that staying in jail does not put prisoners at risk for developing PV. Some similar studies on clinic-epidemiologic features of PV in different populations are presented in [Table - 1]. With regard to these findings, we can propose that there seems to be no difference between pattern of infection in general population and prisoners′ population in the aspects evaluated in this study. However, having a control group from the same city could make us capable of commenting on this subject with more certainty. Therefore, a case-control study on this subject can identify any specificity in the pattern of Malassezia infection in jail if it exists. Acknowledgement The authors would like to thank Farzan Institute for Research and Technology for technical assistance.[33]References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09121t1.jpg] |
| |||||||||


{kind=link}