 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
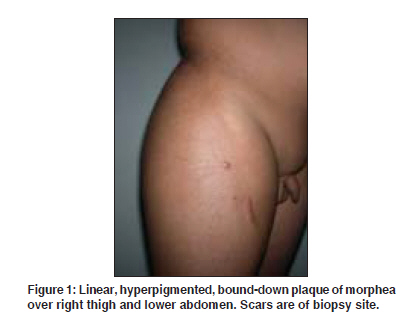
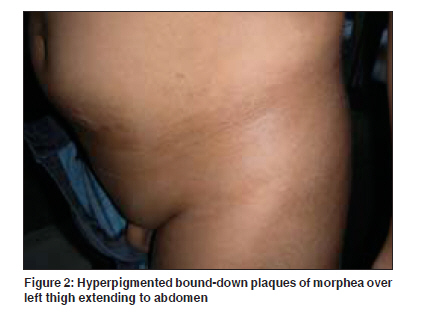
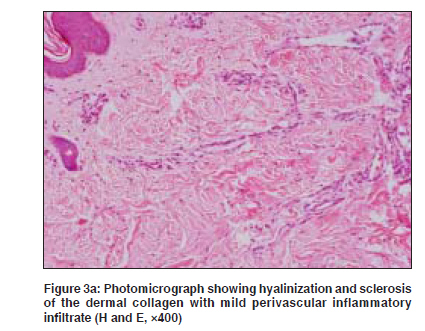
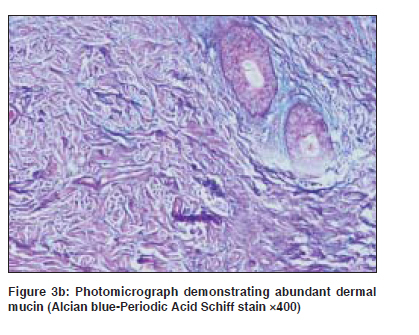
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 388-390 Case Report Linear morphea with secondary mucinosis Khandpur Sujay, Singh Saurabh, Sharma VinodK, Gupta Ruchika, Singh ManojK Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi Code Number: dv09149 PMID: 19584465 Abstract Secondary mucin deposition in the skin is a common feature of lupus erythematosus and dermatomyositis. In scleroderma, it occurs uncommonly or in small amount. We describe a 7-year-old boy with progressive, linear, bound-down plaques involving the thighs, lower abdomen and back with no systemic involvement. Histopathology showed features of scleroderma with abundant mucin deposition in the reticular dermis. This report highlights excessive mucin deposition in lesions of morphea.Keywords: Morphea, Scleroderma, Secondary mucinosis Introduction Mucin deposition is a common histological feature of various connective tissue diseases such as lupus erythematosus and dermatomyositis. In scleroderma, small and interstitial deposits of mucin are occasionally seen in the deep dermis and interlobular septa of subcutis. [1] There are only isolated reports of scleroderma associated with abundant mucin deposits, manifesting as papules within or occurring beyond the indurated plaque. We describe an unusual case of linear morphea evolving into generalized morphea with excessive mucin deposition, without any systemic involvement.Case Report A 7-year-old boy developed a linear, slowly progressive, bound-down plaque on the right thigh at 18 months of age preceded by MMR (Measles Mumps Rubella) vaccine. Subsequently, he developed similar plaques on the other thigh, lower abdomen and back. He had no systemic complaints. Dermatological examination revealed linear, light brown, well- to ill-defined, bound- down indurated plaques with overlying mild hypertrichosis in isolated plaques only, on lateral aspect of both thighs, lower abdomen and back [Figure - 1] and [Figure - 2]. A diagnosis of linear morphea evolving into generalized morphea was made. Skin biopsy done from outside was reported as cutaneous mucinosis. A repeat skin biopsy performed at our institute showed epidermal atrophy, hyalinization of collagen throughout the dermis and mucin deposition in upper reticular dermis [Figure - 3]a. On alcian blue- Periodic Acid Schiff stain, abundant mucin deposition was demonstrated in the upper reticular dermis [Figure - 3]b. Investigations including hematological, biochemical, serum and urine protein electrophoresis, thyroid function tests and antinuclear antibody (ANA) were normal. A diagnosis of morphea with secondary mucinosis was made and oral mini-pulse steroid therapy with betamethasone, 3mg every Saturday and Sunday initiated. Six months of treatment showed no response and repeat skin biopsies from right thigh and abdominal plaque showed features compatible with scleroderma. The dose of betamethasone was increased to 4 mg but with no improvement. Discussion This is an unusual case of linear morphea with abundant mucin deposition. Mucin deposition is a constant feature in both morphea and systemic sclerosis as shown in some case series. [1],[2] In such cases, the amount of mucin is usually mild, rarely evident on routine stains and located mainly in the deep reticular dermis and interlobular septa of subcutis. The deposits chiefly consist of dermatan sulfate and hyaluronic acid. However, there are only isolated reports of localized (linear) or generalized morphea with remarkable mucin deposition. [3],[4],[5] In fact in a few cases, this led to development of papules, nodules and plaques of cutaneous mucinosis both within and distant from the sclerotic areas. None of them had systemic involvement. Pathogenic mechanisms for the production of mucin in scleroderma implicate the role of transforming growth factor-b, which stimulates fibroblasts to produce increased amount of glycosaminoglycans, fibronectin and collagen, decreases extracellular matrix break down and reduces fibroblast susceptibility to apoptosis.[6] Similarly, the role of CD4+ T cells, plasma cells and histiocytes, all of which may stimulate dermal fibroblasts, has also been postulated. Our case must be differentiated from four patients reported by Prendiville et al . who presented with hyperpigmented and hypertrichotic plaques, which were also indurated in two cases, over the lower trunk, buttocks, genitalia and lower limbs with associated multisystemic involvement in the form of proptosis of the eyes, hepatosplenomegaly, paraortic lymphadenopathy, diabetes, dysmorphic features and cardiovascular abnormalities and histopathology showing benign dermal perivascular and interstitial infiltrate composed of lymphocytes, histiocytes and plasma cells with mild subcutaneous infiltrate, hyalinization of collagen in reticular dermis including fibrosis and increased mucin in between collagen bundles. [7] POEMS syndrome can also present with cutaneous changes of diffuse hyperpigmentation, thickening and sclerodermoid changes, diffuse hypertrichosis more prominent on face, chest and limbs, plethora, hemangiomata (glomeruloid hemangioma) and white nails. Diagnosis of POEMS syndrome requires two major features which include polyneuropathy and monoclonal plasma cell proliferative disorder and one minor feature such as sclerotic bone lesions, Castleman′s disease, organomegaly (splenomegaly, hepatomegaly or lymphadenopathy), edema (edema, pleural effusion or ascites), endocrinopathy (adrenal, thyroid, pituitary, gonadal, parathyroid, pancreatic), skin changes or papilledema. [8] Our patient showed linear bound-down plaques over lower trunk and thighs with mild hypertrichosis in isolated plaques only, no systemic involvement and histopathology showing abundant mucin deposition in upper reticular dermis with diffuse sclerosis of collagen. We also excluded other cutaneous mucinosis such as scleredema and scleromyxedema. Scleredema manifests as sudden onset symmetric induration of skin usually preceded by prodrome of fever, body aches and an identifiable focus of infection. Histology reveals collagen bundles separated by large interfascicular space due to mucin deposition. In scleromyxedema, there are small clustered papules and diffuse plaques with constant facial involvement and usually associated with paraproteinemias. In contrast to scleroderma, skin is pinchable and moveable over the subcutis. Deposition of mucin occurs in the papillary dermis. Other dermatoses with secondary mucinosis include connective tissue diseases like lupus erythematosus (LE) and dermatomyositis, malignant atrophic papulosis and certain skin tumors like neural, mesenchymal and epithelial tumors. [3] Our patient did not respond to long-term steroid therapy. In the case of generalized morphea with papular mucinosis reported by Rongioletti et al ., the sclerotic plaques did not improve and new ones continued to appear despite being on prednisone 25mg daily. [5] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09123f2.jpg] [dv09123f3b.jpg] [dv09123f3a.jpg] [dv09123f4.jpg] [dv09123f3.jpg] [dv09123f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}