 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
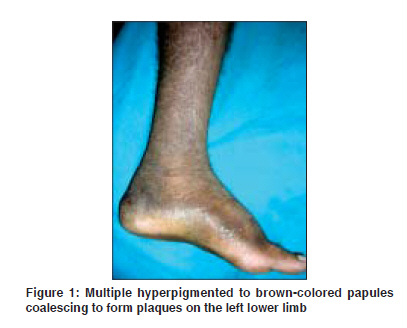
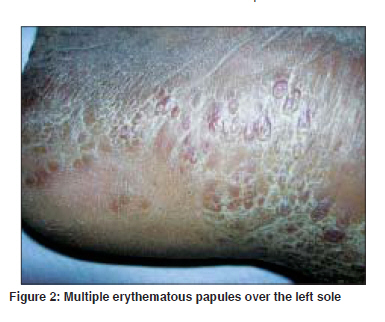
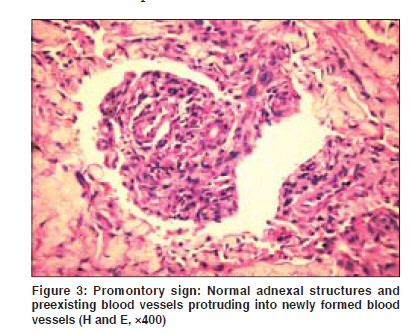
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 391-393 Case Report Kaposi's sarcoma: A presenting manifestation of HIV infection in an Indian Kharkar V, Gutte Rameshwar M, Khopkar U, Mahajan S, Chikhalkar S Department of Dermatology, Seth G.S. Medical College and King Edward Memorial Hospital, Mumbai Code Number: dv09150 PMID: 19584466 Abstract Kaposi's sarcoma (KS) is a multifocal neoplastic proliferation of endothelial cells predominantly involving skin and other organs. HIV-associated Kaposi's sarcoma has been rarely reported from India. A 38-year-old male presented with persistent swelling on the left lower limb for one year along with multiple erythematous to dusky papules and plaques of one and half months duration and swelling and black discoloration of right lower limb for one month. Cutaneous examination revealed numerous skin colored and erythematous papules and plaques distributed on the left lower limb on the anteromedial aspect and verrucous plaque on the left sole. Multiple erythematous, grouped papules were present over the soft palate. Skin biopsy showed numerous slit like spaces dissecting into the collagen of the upper and mid-dermis along with 'promontory sign' suggestive of Kaposi's sarcoma. Patient was found to be HIV-positive by ELISA test.Keywords: Kaposi′s sarcoma, HIV, India Introduction Kaposi′s sarcoma (KS) is a multifocal neoplastic proliferation of endothelial cells involving skin and other organs. Despite high prevalence of HIV/AIDS in India, Kaposi′s sarcoma affecting skin and mucus membranes has been rarely reported and only nine such cases exist in the published literature from India. [1] We report Kaposi′s sarcoma as a presenting manifestation of HIV infection in a heterosexual male from India.Case Report A 38-year-old married male presented with persistent swelling of the left lower limb for one year, swelling of right foot for one month, multiple red raised lesions on left lower limb for one and a half month along with black discoloration on right lower limb of one month duration. There was no history of trauma, fever with chills, weight loss, genital lesions or blood transfusion prior to onset of lesions. He denied history of extramarital and premarital sexual exposure. There was a past history of pulmonary tuberculosis ten years ago and he had taken incomplete treatment. He relapsed recently with pulmonary tuberculosis for which he was put on second-line antituberculous therapy. Cutaneous examination showed multiple skin colored to erythematous compressible papules coalescing to form plaques on the left lower limb along with multiple soft compressible tender papules on the left sole spreading in linear fashion [Figure - 1] and [Figure - 2]. There was non-pitting edema of the left lower limb with oozing of serous fluid suggestive of lymphatic edema. He also had multiple erythematous papules over the soft palate along with multiple erythematous plaques over the left side of chest, buttocks and forearm. There was no lymphadenopathy. Systemic examination was normal except for rales over the right suprascapular area. A clinical diagnosis of Kaposi′s sarcoma was suspected. After pre-test counseling, the patient was advised ELISA test for HIV which turned out to be positive. Laboratory investigations revealed hemoglobin: 11.43 gm%, total leukocyte count: 4500 (P85%, L14%, E1%), red blood cells: 2.94 million/mm 3 , platelets: 1,20,000/mm 3 , erythrocyte sedimentation rate: 62 mm at the end of one hour. Stool for occult blood was negative. Serum alkaline phosphatase was 46 IU/L (normal 40-120 IU/L). Sputum was positive for acid-fast bacilli (AFB). VDRL was reactive (1 : 16 titers) but TPHA was negative, Mantoux test was positive (12 mm). His absolute CD4 count was 115/mm 3 (normal 337-1513) and CD8 count was 1336 mm 3 (normal 174-1240). Viral markers for hepatitis B and C were negative. Polymerase chain reaction (PCR) for human herpesvirus 8 (HHV-8) could not be done because of lack of facilities. A chest X-ray showed right apical fibrocavitatory lesion suggestive of pulmonary tuberculosis. A skin biopsy of the representative skin lesion showed numerous slit-like spaces formed by vascular channels dissecting into the collagen of upper and mid-dermis. There was extravasation of RBCs with a moderate superficial and deep perivascular lymphocytic infiltrate along with promontory sign (a small vessel protruding into an abnormal vascular space) [Figure - 3]. Gram stain and AFB stain were negative for organisms. A diagnosis of Kaposi′s sarcoma (KS) was made. Immunohistochemical markers viz., CD31, CD34 and factor VIII were positive. Ultrasonography of the abdomen demonstrated diffuse hypoechoic liver (probably due to drug-induced hepatitis) with paraaortic and mesenteric lymphadenopathy. According to NACO guidelines, Highly active antiretroviral therapy (HAART) was not started as the patient was on antituberculous therapy. One and half month later, he was readmitted with complaints of dyspnea and recurrent attacks of hemoptysis. Computed tomography (CT) scan of the chest revealed a single large necrotic cavitatory lesion in the right apical region but no evidence of pulmonary involvement by KS. Repeat sputum AFB was positive after five months of antituberculous therapy, therefore category II antituberculous therapy was started along with HAART. Discussion Kaposi′s sarcoma is reported as the initial manifestation of the AIDS syndrome in approximately 30% of cases. The first report of AIDS-associated KS from India was in 1993 in a 35-year-old female sex worker. She had multiple painless non-pruritic nodules of varying colors on the right leg with swelling of leg. Since then, a very few cases had been reported amongst Indian patients. In 1996, Kumarasamy et al . reported cutaneous KS in a HIV-positive intravenous drug abuser. [2] Chandan et al . reported AIDS-associated KS with purpuric macules, lichenoid papules and plaques and hyperkeratotic violaceous nodules with mucosal and genital involvement in a heterosexual male. [3] In the early 1980s, epidemic form of KS was detected in homosexual mens in urban areas of New York and California. This was recognized to be associated with a new retrovirus HIV-1. Up to 30% of those infected men developed KS. [4] In patients with other modes of HIV transmission, the prevalence of KS was less than 5%. [5] Epidemiological studies suggest that HIV did not spread to India until the year, 1985. By 1990, several studies in Mumbai reported a high prevalence of HIV infection. [6] Initial reports described it in homosexual men with AIDS, but recent publications have also reported its occurrence in heterosexual males. [3],[7] Among cases reported in India, two were heterosexual males. Present report is of KS in an HIV-positive heterosexual male. AIDS-related KS usually presents with cutaneous and mucus membrane lesions, or lymph node involvement. Visceral involvement occurs in 50% of the patients, especially of lungs and gastrointestinal tract. Lung involvement occurs in 20% of the patients and is the most life-threatening form of the disease.[8] Involvement of lower limbs in HIV-associated KS appears to be a rule rather than exception in Indian cases. In treatment of HIV-associated KS, HAART forms the mainstay of treatment. Along with HAART, liposomal anthracyclines like doxorubicin are considered as first line systemic therapy for KS because of their good clinical response and relatively few side effects. Paclitaxel is an alternative agent that can induce remission in persons who relapse after anthracycline therapy. [9] In countries unable to afford cost of HAART, treatment of KS is likely to be palliative at best. [10] In absence of HAART, etoposide was found to be more effective than supportive care or radiotherapy. [11] The HIV-associated KS usually gets disseminated to the skin, visceral organs and lymph nodes. Common causes of death in AIDS-associated KS are intercurrent illness and systemic involvement especially of the pulmonary system. The cause of low prevalence of KS in our country may be due to low prevalence of HHV-8 in our country. [12] We report this case for its rarity and occurrence of KS as the presenting manifestation of asymptomatic HIV disease even at low CD4 count in a heterosexual male. Acknowledgment We gratefully acknowledge the help of Dr. S. Gujral, Department of Pathology, Tata Memorial Hospital, Mumbai for arranging immunohistochemistry studies for our patient. We also gratefully acknowledge the help of Dr. D. G. Saple for his valuable guidance. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09124f1.jpg] [dv09124f2.jpg] [dv09124f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}