 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
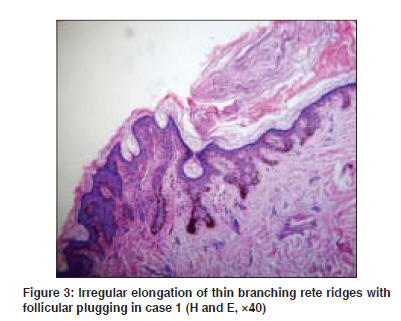
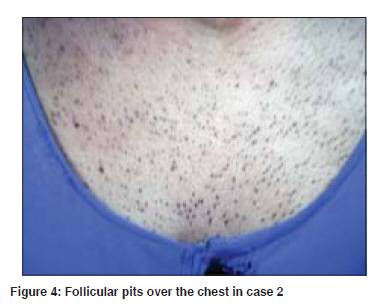
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 398-400 Case Report Three cases of Dowling Degos disease in two families Bhagwat PV, Tophakhane RS, Shashikumar BM, Noronha TonitaM, Naidu Varna Department of Skin and STD, Karnataka Institute of Medical Sciences, Hubli, Karnataka Code Number: dv09152 PMID: 19584468 Abstract Dowling Degos disease is a rare condition inherited as autosomal dominant trait characterized by numerous, asymptomatic, symmetrical, progressive, small, round-pigmented macules over axillae and groins, face, neck, arms and trunk, scattered comedo-like lesions (dark dot follicles) and pitted acneiform scars. Histopathology is diagnostic. We are hereby reporting three cases of Dowling Degos disease belonging to two families. Our first and second case belonged to the same family, whereas our third case belonged to different family. In our series, all the patients had onset after puberty. All three cases had reticulate pigmentation over face and/or flexures, black comedones and follicular pits. On histopathological examination of the skin biopsy taken from the lesion over the back, all these patients showed classical histopathological features of Dowling Degos disease. We feel that one should investigate the patient presenting with reticulate pigmentation over the face and flexures with blackish comedone-like lesions, because histopathological features of this condition are unmistakable.Keywords: Dowling Degos disease, Reticulate pigmentation, Pigmented comedones Introduction Dowling Degos disease, also described in the literature as reticular pigmented anomaly of flexures, is a rare, benign genodermatosis, inherited as autosomal dominant trait. Onset is usually in the adulthood. The disease is characterized by numerous, asymptomatic, symmetrical, progressive, small, round-pigmented macules over axillae and groins, face, neck, arms and trunk, scattered comedo-like lesions (dark dot follicles) and pitted acneiform scars. Histopathology is diagnostic with a distinctive form of acanthosis, characterized by an irregular elongation of thin branching rete ridges, with a concentration of melanin at the tips. In some cases, there is follicular plugging. The clinical and histopathological changes were memorably summarized by Wilson-Jones and Grice as ′demonstrating dusky dappled disfigurements and dark dot depressions and disclosing digitate downgrowths delving dermally′. [1] Because of its favorable prognosis, differentiation of this benign disorder from acanthosis nigricans, a cutaneous marker of possible or existing internal malignant disease, is highly important. Careful clinical examination of lesions in correlation with characteristic histopathological features makes the diagnosis simple and straightforward. [2]Case Reports Case 1 Her general physical examination and systemic examinations were normal. Cutaneous examination revealed multiple pits varying in size from 1-3 mm and open comedone-like lesions distributed over the cheeks, chin, neck, back, chest and abdomen. There was diffuse, reticulate pigmentation of the face, neck and upper trunk [Figure - 1] and [Figure - 2]. Mucosae, hair and nail, flexures, scalp and palms and soles were normal. On investigation, complete hemogram, liver and renal function tests were all within normal limits. Biopsy was done from a lesion over the back and histopathological examination revealed hyperkeratosis, acanthosis, irregular elongated thin branching rete ridges growing down into the dermis, plugging of pilosebaceous orifice with keratin and increased melanin pigment in the lower part of rete pegs [Figure - 3]. Case 2 A sixteen year old female (daughter of case one) presented with hyperpigmented skin lesions over the face, chest and back for two years. The eruption first started over the face, gradually progressed to involve the chest and back. Patient gave history that some black material forms in the pits over a period of three to four months and then falls on its own to again form fresh black material. There was no history of erythema of the face. There was no significant past medical or surgical history. Patient′s grandfather, mother, aunt and two brothers were affected with the same disease. Her general physical examination and systemic examinations were within normal limits. Cutaneous examination revealed diffuse, black, comedone-like lesions distributed over the forehead, cheeks and neck with multiple pits over the upper chest and back. Trunk was more severely affected when compared to the face and neck [Figure - 4]. There was reticulate pigmentation over the flexures. Few nodular cysts were also noted over the back. Rest of the cutaneous examination was normal. All relevant investigations were within normal limits. Biopsy was done from the representative skin lesion over the back which revealed elongated rete ridges with increased melanin pigment in the lower part of the rete ridges and plugging of pilosebaceous orifice with keratin. Case 3 A 27-year-old male, resident of Hubli, Karnataka, presented to us with asymptomatic skin eruptions over the back since the age of 14 years. Initially, lesions were raised above the skin surface and small. Gradually, these lesions progressed to form pits filled with blackish material. Gradually, he developed similar lesions over the face and chest over the next one year. He had no history of facial erythema. There was no significant past medical or surgical history. The patient was born of non- consanguineous marriage. His grandmother (78-year-old), father (50-year-old), elder brother (29-year-old) and his younger brother (26-year-old) were affected with the same disease. Cutaneous examination revealed multiple pits of varying sizes, distributed over the upper back, upper chest, arms, cubital fossae and over forearms. There was diffuse reticulate pigmentation over the cubital fossae, axillae, inguinal region and face. Rest of the cutaneous examination was unremarkable. Routine blood investigations, urine investigations, biochemical parameters were all within normal limits. Skin biopsy was done from the lesion over the back and subjected to histopathological examination which revealed hyperkeratosis, elongation of rete ridges with increased melanin pigment at the lower part of rete ridges and keratotic plugging of the pilosebaceous orifice. All of our patients were treated with topical retinoids and oral isotretinoin 20 mg daily for two months. Our first and second patients were counseled before isotretinoin therapy. There was not much of improvement in lesions and hence the oral isotretinoin was discontinued and topical retinoids were continue. Discussion Dowling Degos disease, the most fascinating skin condition, has very characteristic clinical and histopathological features. The diagnosis is very simple when classical features are present as seen in our cases. We had considered the differential diagnosis of familial dyskeratotic comedones, acne conglobata and follicular occlusion tetrad. But all of our patients had distinctive black comedones, follicular pits and reticulate pigmentation in addition to nodulocystic lesions. There was family history suggestive of autosomal dominant inheritance. All of our patients showed very characteristic histopathological features. The diagnosis of follicular occlusion tetrad was ruled out because none of our patients had lesions suggestive of hidradenitis suppurativa, pilonidal sinus or dissecting cellulitis of the scalp. In a case report, 15 members of a large family had Dowling Degos disease out of which, the authors examined five members. In their series, the study of the family tree supported autosomal dominant transmission with female preponderance. The authors also noted unusual features such as acral distribution of lesions, palmar pigmentation and seborrheic keratosis like lesions. [3] In other case reports also, there was female preponderance. [4],[5],[6],[7] In another case report, authors did not find any seborrheic keratosis like lesions, pin head sized pigmented comedones and pitted follicular pores. [8] In our series, we noted autosomal dominant inheritance and out of three cases we have seen, two patients were females. We did not find seborrheic keratosis like lesions in our patients but we have noted pin head sized pigmented comedones and pitted follicular pores. In another case report, a 61-year-old male presented with persistent rosacea like rash over forehead, cheeks, chin and nose, small follicular papules, scaly nodules and depressed scars on the trunk and limbs. Histopathological features resembled that of Dowling Degos disease. This condition has been named as Haber′s syndrome. [9] Our patients did not have any rosacea-like eruption. These cases have been reported because there are a very few reports both in Indian and Western literature. We had these three cases in the last two years and we feel that the condition is not as rare as reported in the literature. Probably, these cases are under-reported. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09126f3.jpg] [dv09126f1.jpg] [dv09126f4.jpg] [dv09126f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}