
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 4, 2009, pp. 410-412
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 410-412
Letter to the Editor
Proximal subungual onychomycosis caused by Aspergillus flavus in a HIV-positive patient
Choudhary SanjivV, Koley Sankha, Mallick Sanjay, Bose Seema, Basak Silpi
Department of Dermatology, Jawaharlal Nehru Medical College, Sawangi, Mahrasthra
Correspondence Address: Dr. Sanjiv V. Choudhary, 28, Modern Nagpur Society, Chhatrapati Nagar, Nagpur - 15 (M.S)
Sanjiv_choudhary26@yahoo.com
Code Number: 09132
PMID: 19584475
DOI: 10.4103/0378-6323.53152
Sir,
Onychomycosis is defined as a fungal infection of the nail caused by dermatophytes, nondermatophyte moulds (NDM) and yeasts. Types of onychomycosis are distal-lateral subungual onychomycosis (DLSO), proximal subungual onychomycosis (PSO), white superficial onychomycosis and total dystrophic onychomycosis. D0 LSO is the most common clinical type. PSO is uncommon in the general population but is frequently associated with human immunodeficiency virus (HIV) infection and is mostly caused by Trichophyton rubrum and Trichophyton megninii . PSO is nearly pathognomonic of HIV infection. [1],[2] Multiple fungal species and unusual opportunistic fungi are frequently cultured from HIV-infected patients and may be a reflection of the degree of immunosuppresion. [3] Previously regarded as contaminants, yeasts and moulds are now being increasingly recognized as pathogens in fungal nail infection. [4] Aspergillus flavus is a widespread saprophyte found in soil, seeds, fruits and decaying vegetation. We report a rare case of PSO caused by Aspergillus flavus in an HIV-positive patient.
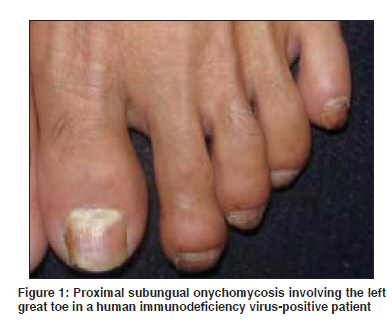
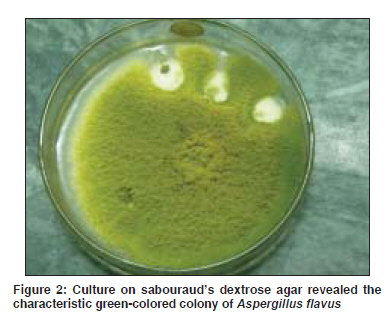
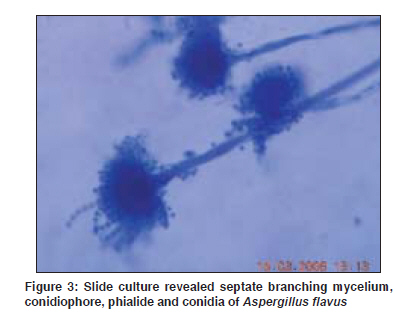
A 30-year-old male patient, farmer by occupation, presented with severe tingling sensation and burning pain affecting both the lower extremities for the past 2 months. He gave history of unprotected heterosexual genito- genital exposure and loss of weight for the past 1.5 years. General examination revealed thin, cachexis built of the patient. Cutaneous examination revealed diffuse greasy scales involving the scalp, eyebrow and retroauricular region. The oral mucous membrane showed a curdy-white plaque involving the dorsum of the tongue. The left great toe nail revealed whitish discoloration of the proximal nail plate with brittleness [Figure - 1]. Nail folds were normal. Clinically, the possibility of Hansen′s disease was ruled out. With this history and clinical examination, the possibility of underlying immunosuppresion was thought and the case was investigated. Routine investigations revealed gross anemia . Blood sugar levels were normal. Enzyme-linked immunosorbent assay test was positive for HIV antibodies. The proximal nail plate of the left great toe was scraped and pared with surgical blade no. 15. With the help of a curette, material from the proximal nail bed was taken. The sample was sent to the microbiology department for KOH examination and culture. KOH examination revealed septate branching mycelium. Culture carried out on Sabouraud′s dextrose agar with chloramphenicol revealed the characteristic green-colored colony suggestive of Aspergillus flavus [Figure - 2]. Slide culture revealed septate branching mycelium, conidiophore, phialide and conidia of Aspergillus flavus [Figure - 3]. Fruiting bodies of Aspergillus flavus are similar to Syncephalastrum racemosum , but Syncephalastrum racemosum has aseptate hyphae and a merosporangial sac surrounding the sporangiospores. KOH examination of the curdy-white plaque from the dorsum of the tongue revealed budding yeast-like cells with pseudohyphae. The final diagnosis was peripheral neuropathy with seborrhoeic dermatitis, oral candidiasis and PSO due to Aspergillus flavus of the left great toe in an HIV-positive patient.
Nondermatophyte moulds (NDM) were the rare cause of onychomycosis. Tosti et al. in their study found that PSO was the most common type of onychomycosis caused by NDM and that those cases were not associated with significant systemic illness or immunosuppresion. [5] Goettmann-Bonvallot, in his article, reported that PSO without fingernail or toenail paronychia is generally caused by Trichophyton rubrum in immunodepressed subjects (patients with acquired immunodeficiency syndrome). [6] Recently published reports from India revealed increased incidence of NDM causing onychomycosis in HIV-infected patients. [7] Several authors have reported cases of onychomycosis due to Aspergillus species. To the best of our knowledge, there are only few reports of Aspergillus flavus (green mould) causing onychomycosis. [8],[9],[10] In our case, Aspergillus flavus species was the pathogen and not a contaminant as (1) KOH examination of nail scrapings revealed a septate branching mycelium, (2) three repeated cultures performed on Sabouraud′s dextrose agar with chloramphenicol revealed characteristic morphology and color suggestive of Aspergillus flavus and (3) slide culture findings were suggestive of Aspergillus flavus only.
PSO is more frequently seen when the CD4 cell count falls below 450 cells/mm 3 . [11],[12] But we did not have follow-up of the patient and CD4 cell counts. Usually, periungual inflammation is seen in onychomycosis (especially PSO) caused by Aspergillus species. [5] But in our case no periungual inflammation was seen. So far, we know that onychomycosis caused by Aspergillus flavus species is a rare finding. To the best of our knowledge, there are only few reports in the international literature and not a single one from India.
Acknowledgment
The authors would like to acknowledge Dr. Priyesh Jaiswal, 3 rd year MD resident of Medicine of Jawaharlal Nehru Medical College, Sawangi.
References
| 1. | Prose NS, Abson KG, Scher RK. Disorders of the nails and hair associated with human immunodeficiency virus infection. Int J Dermatol 1992;31:453-7. Back to cited text no. 1 [PUBMED] |
| 2. | Sehgal VN, Join S. Onychomycosis- clinical perspective. Int J Dermatol 2000;39:241-9. Back to cited text no. 2 |
| 3. | Cribier B, Mena ML, Rey D, Partisani M, Fabien V, Lang JM, et al . Nail changes in patients infected with human immunodeficiency virus. A prospective controlled study. Arch Dermatol 1998;134:1216-20. Back to cited text no. 3 |
| 4. | Midgley G, Moore MK, Cook C, Phan QG. Mycology of nail disorders. J Am Acad Dermatol 1994;31:S68-74. Back to cited text no. 4 |
| 5. | Tosti A, Piraccini BM, Lorenzi S. Onychomycosis caused by nondermatophytic molds: Clinical features and response to treatment of 59 cases. J Am Acad Dermatol 2000;42:217-24. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Goettmann-Bonvallot S. Clinical types of onychomycosis. Ann Dermatol Venereol 2003;130:1237-43. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Surjushe A, Kamath R, Oberai C, Saple D, Thakre M, Dharmshale S, et al . A clinical and mycological study of onychomycosis in HIV infection. Indian J Dermatol Venereol Leprol 2007;73:397-401. Back to cited text no. 7 [PUBMED]  |
| 8. | Gianni C, Romano C. Clinical and histological aspects of toenail onychomycosis caused by Aspergillus spp. Dermatology 2004;209:104-10. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Mahmoudabadi AZ, Zarrin M. Onychomycosis with Aspergillus flavus : A case report from Iran. Pak J Med Sci 2005;21:497-8. Back to cited text no. 9 |
| 10. | Hilimoglu-Polat S, Metin DY, Inci R, Dereli T, Kilinc I, Tumbay E. Nondermatophyte molds as agents of onychomycosis in Turkey: A prospective study. Mycopathologica 2005;160:125-8. Back to cited text no. 10 |
| 11. | Kaplan MH, Sadick N, McNutt NS, Meltzer M, Sarngadharan MG, Pahwa S. Dermatologic findings and manifestations of AIDS. J Am Acad Dermatol 1987;16:485-506. Back to cited text no. 11 [PUBMED] |
| 12. | Conant MA. The AIDS epidemic. J Am Acad Dermatol 1994;31:47-50. Back to cited text no. 12 |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09133f2.jpg]
[dv09133f3.jpg]
[dv09133f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}