
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 4, 2009, pp. 412-414
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 412-414
Letter to the Editor
Acral dyschromatosis with developmental regression and dystonia in a seven- year-old child: Dyschromatosis symmetrica hereditaria variant or a new syndrome?
Kaliyadan Feroze, Vinayan KP, Fernandes Bindiya, Jayasree MG
Department of Dermatology, Amrita Institute of Medical Sciences, Kochi, Kerala - 682 028
Correspondence Address:Dr. Feroze Kaliyadan, Department of Dermatology, Amrita Institute of Medical Sciences, Kochi, Kerala - 682 028
ferozkal@hotmail.com
Code Number: 09133
PMID: 19584476
DOI: 10.4103/0378-6323.53154
Sir,
A 7-year-old girl, born to non-consanguineous parents was referred to us from the Pediatric Neurology department for evaluation of pigmentary changes over the face and extremities. The patient was being evaluated under neurology for progressive regression of developmental milestones, associated with feeble vocalization, difficulty in walking and dystonic posturing, all of which apparently developed after the age of about one and half years. Child also had ptosis of the left eye since birth, which did not show any diurnal variation. There was no definite history of seizures. The patient′s parents noticed hypopigmented and hyperpigmented patches initially over both hands, followed by involvement of foot and face since around the age of one year. There was no history of any tendency to itch or scratch and there was no history suggestive of photo-exacerbation. There was no history of any other significant skin or mucosal lesion or of any hair, nail and teeth abnormalities. There was no significant family history of any skin or neurological disorders.
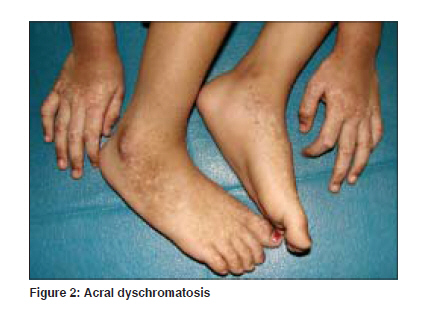
On examination, the patient had a dysmorphic facies with long philtrum, and thin upper lip. Dermatological examination revealed hypopigmented and hyperpigmented macules grouped over the dorsum of hands and feet and over the face [Figure - 1] and [Figure - 2]. There was no evidence of leuko-trichia over the hypopigmented lesions. The skin did not reveal atrophy or telangiectasia. No other significant skin or mucosal lesions were seen. Hair, teeth and nails were normal.
Significant findings on neurological examination included - left partial ptosis with Marcus Gunn phenomena. Dystonic posturing of right upper extremity was seen with spasticity of left lower limb. The patient also had an awkward gait with short steps and narrow base and also had a prominent knock-knee and bilateral pes plano-valgus. There were no other significant skeletal system abnormalities.
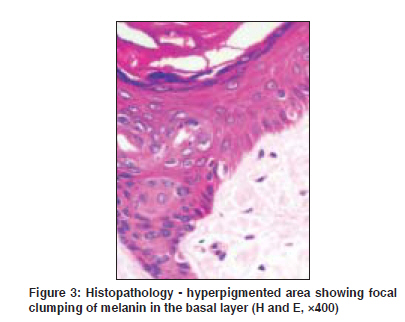
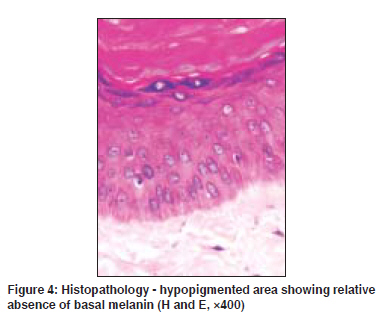
Laboratory investigations, including blood work-up, screening for metabolic disorders and karyotyping were normal. MRI of the brain was normal except for symmetrical hyperintensities in bilateral putamen. EEG was essentially normal. Skin biopsy from the hypopigmented areas showed a marked absence of basal melanin while the hyperpigmented lesion showed increased focal melanin pigmentation [Figure - 3] and [Figure - 4]. Based on the clinical features and the investigation findings, a diagnosis of symmetrical acral dyschromatosis (to rule out dyschromatosis symmetrica hereditaria) was considered.
Dyschromatosis symmetrica hereditaria (DSH) or reticulate acropigmentation of Dohi is characterized by hyperpigmented and hypopigmented macules on the face and dorsal aspects of the extremities that appear in infancy or early childhood. DSH has been more commonly reported in Japanese and Chinese patients and is inherited in an autosomal-dominant pattern. Various mutations of the RNA-specific adenosine-deaminase gene (DSRAD) also known as adenosine deaminase, RNA-specific (ADAR), have been reported in DSH. [1],[2],[3]
There have been very few significant non-cutaneous associations reported with DSH. Significantly though there have been two reports of associated dystonia. Tojo et al. reported DSH in a family associated with dystonia and mental deterioration. [4] Patrizi et al. reported a case associated with idiopathic torsion dystonia. [5]
Dyschromatosis symmetrica hereditaria needs to be differentiated from dyschromatosis universalis hereditaria (DUH), which is characterized by more extensive lesions including the non-acral/unexposed areas of the skin. A segmental variant called unilateral dermatomal pigmentary dermatosis (UDPD) has also been described. [6] Some of the differential diagnosis of dyschromatosis which needs to be generally considered includes xeroderma pigmentosum, dyschromic amyloidosis and exposure to chemicals such as diphenylcyclopropenone and monobenzyl ether of hydroquinone. [7]
In our case, there was symmetrical dyschromatosis in an acral distribution associated with regression of milestones and progressive dystonia. However, unlike typical DSH, the lesions (both hypo and hyperpigmented) were larger in size. We present this case as a possible variant of DSH or a newer syndrome with acral dyschromatosis and neurological features like regression of developmental milestones and dystonia.
References
| 1. | Miyamura Y, Suzuki T, Kono M, Inagaki K, Ito S, Suzuki N, et al . Mutations of the RNA-specific adenosine deaminase gene (DSRAD) are involved in dyschromatosis symmetrica hereditaria. Am J Hum Genet 2003;73:693-9. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Oyama M, Shimizu H, Ohata Y, Tajima S, Nishikawa T. Dyschromatosis symmetrica hereditaria (reticulate acropigmentation of Dohi): Report of a Japanese family with the condition and a literature review of 185 cases. Br J Dermatol 1999;140:491-6. Back to cited text no. 2 [PUBMED] [FULLTEXT] |
| 3. | Kondo T, Suzuki T, Mitsuhashi Y, Ito S, Kono M, Komine M, et al . Six novel mutations of the ADAR1 gene in patients with dyschromatosis symmetrica hereditaria: Histological observation and comparison of genotypes and clinical phenotypes. J Dermatol 2008;35:395-406. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Tojo K, Sekijima Y, Suzuki T, Suzuki N, Tomita Y, Yoshida K, et al . Dystonia, mental deterioration, and dyschromatosis symmetrica hereditaria in a family with ADAR1 mutation. Mov Disord 2006;21:1510-3. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Patrizi A, Manneschi V, Pini A, Baioni E, Ghetti P. Dyschromatosis symmetrica hereditaria associated with idiopathic torsion dystonia. A case report. Acta Derm Venereol 1994;74:135-7. Back to cited text no. 5 |
| 6. | Rai R, Kaur I, Handa S, Kumar B. Dyschromatosis Universalis Hereditaria. Indian J Dermatol Venereol Leprol 2000;66:158-9. Back to cited text no. 6  |
| 7. | Urabe K, Hori Y. Dyschromatosis. Semin Cutan Med Surg 1997;16:81-5. Back to cited text no. 7 [PUBMED] |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09134f3.jpg]
[dv09134f2.jpg]
[dv09134f1.jpg]
[dv09134f4.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}