
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 4, 2009, pp. 414-416
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 414-416
Letter to the Editor
Ross syndrome
Metta ArunKumar, Athanikar SB, Ramachandra S, Mohammad Shibu
Department of Dermatology, Venereology and Leprology, Kamineni Institute of Medical Sciences, Narketpally, Nalgonda - 508 254, AP
Correspondence Address:Dr. Arun Kumar Metta, Department of Dermatology, Venereology and Leprology, Kamineni Institute of Medical Sciences, Narketpally, Nalgonda - 508 254, AP
drmettaarun@yahoo.co.in
Code Number: 09134
PMID: 19584477
DOI: 10.4103/0378-6323.53156
Sir,
Ross syndrome is a rare disorder of sweating associated with depressed or absent deep tendon reflexes and tonic pupil due to selective degeneration of sympathetic pathways. [1] About 40 cases of Ross syndrome have been reported so far. We report below a 19-year-old patient with typical features of Ross syndrome.
A 19-year-old male patient presented with heat intolerance and absence of sweating from the face, trunk and extremities in an irregular fashion for last 5 years. As the patient was working in a bakery, the ambient temperature of which is high, the patient could not tolerate the atmosphere and used to go out or pour water on his body frequently. But there was no history of hospitalization for hyperthermia at any time. He also noticed that the left half of the face was not sweating as much as the right side. On the trunk, there were patchy areas of increased and decreased sweating. The patient had not applied any topical medication to any part of the body. There was no history of trauma to the spine, syncopal attacks or any other chronic febrile illness.
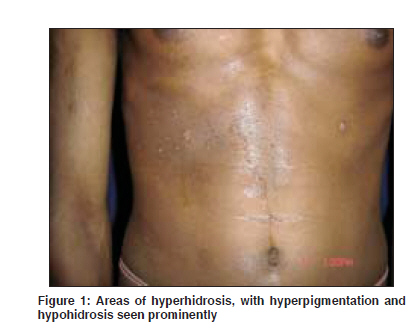
General clinical examination was normal. Blood pressure readings both on supine and prone positions were normal. On cutaneous examination of the left side of the face over the area of the cheek, there was no sweating and the hair in the beard and moustache area were comparatively sparse. There was increased sweating over areas corresponding to T8 and T9 dermatomes on the right side and T3 and T4 dermatomes on the left side [Figure - 1]. The skin over the dermatomes showed uniform hyperpigmentation. The remaining skin over the trunk showed decreased sweating even after vigorous exercise. Both the upper limbs and the lower limbs including the palms and soles showed decreased sweating.
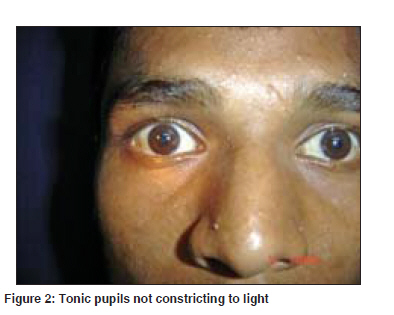
Pupils of both the eyes were sluggish in their reaction to light and on adding 0.125% pilocarpine drops, there was constriction of both the pupils (Holme′s Adie pupil) [2] [Figure - 2].
Ankle reflex, knee reflex, biceps and supinator reflex of both sides were depressed. Other systemic examinations including the central nervous system and spine were normal.
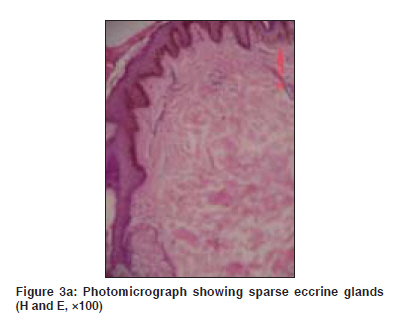
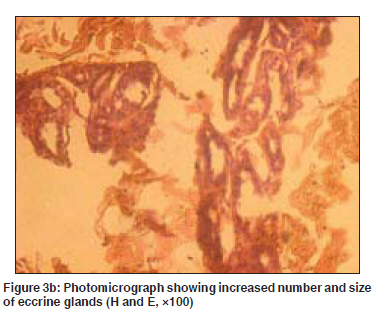
Routine investigations like hemogram, urine examination and thyroid profile were within normal limits. Venereal Disease Research Laboratory (VDRL) test was nonreactive. Chest X-ray and radiographs of the cervical, thoracic and lumbosacral spine detected no abnormality. Histopathological examination from the anhidrotic area showed sparse to absent eccrine sweat glands and the biopsied skin from the hyperhidrotic area showed increased number and size of eccrine sweat glands and epidermal hypermelanosis [Figure - 3]a and b.
Ross syndrome is a rare disorder of sweating comprising of widespread hypohidrosis combined with patchy compensatory hyperhidrosis associated with areflexia and tonic pupil (Holme′s Adie syndrome). [1] It affects both males and females with age of onset ranging from 3 to 50 years. Patients with Holme′s Adie syndrome often show asymptomatic changes in sweating. The anhidrosis may be localized or widespread. When anhidrosis is extensive, the remaining areas of the functioning eccrine glands may show compensatory hyperhidrosis. [2] Cardiac sympathetic denervation that may be asymptomatic has been shown to develop. The compensatory hyperhidrosis may be striking and severe enough to require therapy, although eventually it may be lost as complete anhidrosis develops. [3] It is thought that in anhidrotic areas, there is severe loss of sudomotor fibers and that there is only a slender network of protein gene product immunoreactive fibers not having receptors for vasoactive intestinal peptide immunoreactive or dopamine-β -hydroxylase axons.[4] The hyperhidrosis could be compensatory or due to early loss of cholinergic M2 inhibitor presynaptic autoreceptors. [5]
Our patient had typical areas of hypohidrosis and compensatory hyperhidrosis with weak tendon reflexes and tonic pupil. There were two unusual features in our patient: one was hyperpigmentation corresponding to hyperhidrotic areas and the other was sparse hairs over the left side of the beard and moustache area. Scanning of the available literature does not throw any light on these unusual features. There is no effective therapeutic management for this condition. Heat intolerance may be managed by wearing wet clothing during physical activity in order to prevent hyperthermia and hyperhidrosis to some extent by iontophoresis [6] and botulinum toxin injection. [7] Recently, topical glycopyrrolate was found to be safe and effective in controlling compensatory hyperhidrosis. [8]
Agarwal et al . [9] have reported two cases of Ross syndrome. Sawhney et al . [10] have reported a case that appears to be a variant of Ross syndrome. To the best of our knowledge, this is the third classical case of Ross syndrome to be reported from India.
References
| 1. | Coulson IH. Disorders of sweat glands. In: Burns T, Breathnach S, Cox N, Griffiths C, editors, Rook's Textbook of Dermatology. 7 th ed. Oxford: Blackwell Science Ltd; 2004. p. 45.14 -45.15. Back to cited text no. 1 |
| 2. | Ross AT. Progressive selective sudomotor denervation. A case with coexisting Adie's syndrome. Neurology 1958;8:809-17. Back to cited text no. 2 |
| 3. | Lucy DD Jr, Van Allen MW, Thompson HS. Holmes-Adie syndrome with segmental hypohidrosis. Neurology 1967;17:763-9, 778. Back to cited text no. 3 |
| 4. | Nolano M, Provitera V, Perretti A, Stancanelli A, Saltalamacchia A, Donadio V, et al . Ross syndrome: A rare or a misknown disorder of thermoregulation? A skin innervation study on 12 subjects. Brain 2006;129:2119-31. Back to cited text no. 4 |
| 5. | Ballestero-Diez M, Garcia-Rio I, Dauden E, Corrales-Arroyo M, Garcia-Diez A. Ross syndrome, an entity included within the spectrum of partial disautonomic syndromes. J Eur Acad Dermatol Venereol 2005;19:729-31. Back to cited text no. 5 |
| 6. | Reinauer S, Schauf G, Holzle E. Ross syndrome: Treatment of segmental Compensatory hyperhidrosis with a modified iontophoretic device. J Am Acad Dermatol 1993;28:308-11. Back to cited text no. 6 |
| 7. | Bergmann I, Dauphin M, Naumann M, Flachenecker P, Müllges W, Koltzenburg M, et al . Selective degeneration of sudomotor fibres in Ross syndrome and successful treatment of compensatory hyperhidrosis with botulinum toxin. Muscle Nerve 1998;21:1790-3. Back to cited text no. 7 |
| 8. | Bajaj V, Hannifa M, Reynolds NJ. Use of topical glycopyrrolate in Ross syndrome. J Am Acad Dermatol 2006;55:S111-2. Back to cited text no. 8 |
| 9. | Agarwal US, Bhargava P, Meena R, Bhargava S, Jain RS, Bhargava R. Ross Syndrome-report of 2 cases. The Indian Practioner 1997;50:909-0. Back to cited text no. 9 |
| 10. | Sawhney MP, Sharma YK, Singh N. Segmental anhidrosis with hyporeflexia associated with congenital spinal deformity: A Ross syndrome variant or inverse Horner's syndrome? Indian J Dermatol Venereol Leprol 2004;70:29-32. Back to cited text no. 10 [PUBMED]  |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09135f2.jpg]
[dv09135f1.jpg]
[dv09135f3b.jpg]
[dv09135f3a.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}