 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
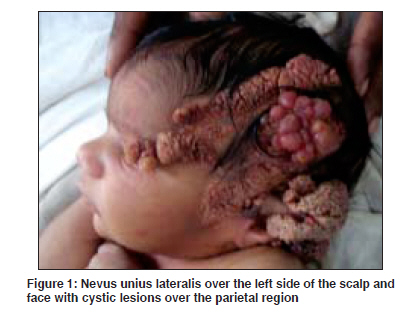
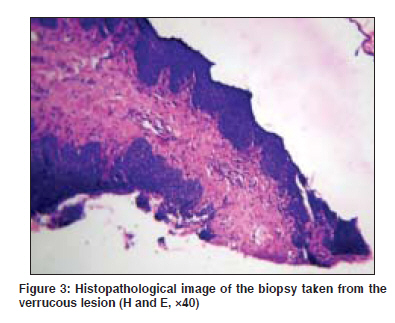
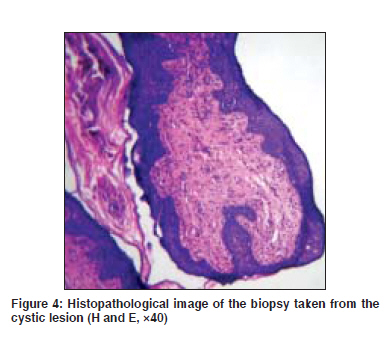
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 419-421 Letter to the Editor Dermatomal giant nevus unius lateralis Bhagwat PV, Tophakhane RS, Shashikumar BM, Naidu Varna Department of Skin and STD, Karnataka Institute of Medical Sciences, Hubli, Karnataka Code Number: dv09164 PMID: 19584480 Sir, Nevus unius lateralis is verrucous epidermal nevus (nevus of one side) arranged in linear fashion in continuous or broken streaks, bands, or patches. The common sites are the trunk and limbs. Verrucous epidermal nevi are rare over the head and neck. There are many reports of nevus unius lateralis associated with abnormalities of the bone and central nervous system like brain tumor and diencephalic syndrome. Histopathology of this nevus shows hyperplastic epidermis chiefly affecting stratum corneum and stratum malpighii. There is variable hyperkeratosis, acanthosis and papillomatosis. [1] We report a case of extensive, dermatomal, nevus unius lateralis present since birth and distributed over the head and neck region, involving the left ear lobe. A 2-month old female baby, born of non consanguineous marriage, full term normal vaginal delivery, presented to us with history of cauliflower like growth over the left side of the scalp and face since the time of birth. There was no history of refusal of feeds, convulsions, excessive cry or vomiting. There was no history of bleeding from the lesion. No other family member was affected with the same disease. On examination, the baby was comfortable and playful. She did not cry on manipulating or touching the lesion. There was a well circumscribed, cauliflower like growth, roughly corresponding to the distribution of the ophthalmic division of trigeminal nerve, encroaching on to the second cervical dermatome on the left side. At two places, the lesion was looking linear in distribution and at other places, it was patchy. The lesion was distributed over the left temporal region, extending on the left parietal region, involving the entire upper half of the left ear lobe, extending to the left side of the forehead and encroaching the whole of the left upper eye lid. The skin lesion was skin colored but at few places, the lesion was bright pink in color and appeared cystic [Figure - 1] and [Figure - 2]. On puncturing one of the cysts, there was oozing of clear, serous fluid. The lesion was soft in consistency and non tender. Clinically, there was no defect in the skull on palpation. There was no bleeding on manipulation. The lesion was not fixed to the underlying structures. Rest of the cutaneous examination was normal. Systemic examination was unremarkable. In view of these findings, we made a clinical diagnosis of nevus unius lateralis. However, we considered epidermolytic hyperkeratosis and verrucous haemangioma as the differential diagnosis. Routine blood and urine investigations, biochemical parameters, X-ray of the skull, computerised scan of the brain were all normal. Skin biopsy was taken from two sites. Histopathological examination of biopsy specimen taken from verrucous lesion revealed hyperkeratosis, acanthosis, papillomatosis, moderate elongation of rete ridges with normal adnexal structures in the dermis [Figure - 3]. There was no proliferation of the capillaries in the dermis. The features were consistent with clinical diagnosis of nevus unius lateralis. The other biopsy was taken from the cystic lesion which on histopathological examination revealed slightly less marked acanthosis. There was no proliferation of capillaries in the dermis. Other findings were similar to the findings of the biopsy taken from the verrucous region [Figure - 4]. Thus a final diagnosis of nevus unius lateralis was made. The baby was shown to pediatric surgeon, who decided to observe the baby and planned the debulking of the lesion later on when the baby grows up. The baby was brought for follow up after two months. At that time, all the cystic lesions were replaced by more solid, verrucous, and vegetative growth. The lesion had become slightly hyper pigmented. The parents were advised to bring the baby for follow up once in every month. Nevus unius lateralis is a type of linear verrucous epidermal nevus which is confined to one side of the body. The common sites are trunk and limbs and involvement of the head and neck region and involvement of the ear lobe is rare. In a study of 4,256 pediatric cases attending the dermatology OPD who were screened for nevi, 16 cases were found to have verrucous epidermal nevi, five of them were linear verrucous epidermal nevi. [2] There was no case of nevus unius lateralis in this report. This indicates that nevus unius lateralis is uncommon condition. Thomas et al . [3] have reported a seven year old girl, with nevus unius lateralis distributed in zosteriform pattern with involvement of the ear lobe. She did not have any systemic abnormalities. [3] There are few similarities between this patient and our patient. Like this patient, our patient also had dermatomal lesion over the left side of the head and neck region with involvement of the left ear lobe and she did not have any systemic abnormalities. But the peculiarity of our patient is that, she had the lesion since birth, and the lesions at few places were cystic, and appeared vascular when we first saw the baby. When the baby came for follow up after two months, the cystic lesions were replaced with more verrucous lesions and vascular appearance was lost. The lesion appeared slightly hyper pigmented. Epidermolytic hyperkeratosis in a systematized linear verrucous epidermal nevus is a rare feature. There are many case reports of such cases, [4],[5] but our patient did not have granular cell degeneration on histopathological examination. The case is being reported for the rarity of the condition and for the unique giant nature in this case. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09138f4.jpg] [dv09138f2.jpg] [dv09138f1.jpg] [dv09138f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}