
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 4, 2009, pp. 422-424
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 422-424
Focus
Leflunomide
Mehta Vandana, Kisalay Saurav, Balachandran C
Department of Skin and STD, Kasturba Hospital, Manipal, Karnataka
Correspondence Address:Department of Skin and STD, KMC, Manipal
vandanamht@yahoo.com
Code Number: dv09165
PMID: 19584481
DOI: 10.4103/0378-6323.53157
Introduction Leflunomide is an isoxazole immuno-modulatory agent which belongs to DMARD (Disease Modifying Antirheumatic Drug) class of drugs. It is an inhibitor of pyrimidine synthesis and has antiproliferative and antiinflammatory actions. Leflunomide was licensed for use in rheumatoid arthritis in 1998 and psoriatic arthritis in 2004.
Structure and Metabolism The chemical name of leflunomide is 5-methyl-N-[4-Triflueromethylphenyl]-5-methylisoxazole- 4-carboxamide. It is a pro-drug and following oral administration is converted to an active metabolite (A77 1726) in the gut wall, plasma and liver; and also to many minor metabolites (of which 4-trifluoromethyaniline is the most important). The parent compound is rarely detected in the plasma. It is the active metabolite A77 1726, which is responsible for all the in vivo activity of leflunomide. [1]
Pharmacokinetics The oral bioavailability of leflunomide is 80% and peak plasma levels of active metabolite are reached 6-12 h after oral administration. The bioavailability of A77 1726 is not affected by high fat meal. As the active metabolite is 99% plasma protein bound, it has a low volume of distribution and hence, the time duration for the effect to start is between 8 and 12 weeks. A77 1726 undergoes enterohepatic circulation and biliary recycling and this may contribute to long elimination half-life (>2 weeks) of the active metabolite. [2]
Mechanism of Action
Antiproliferative action
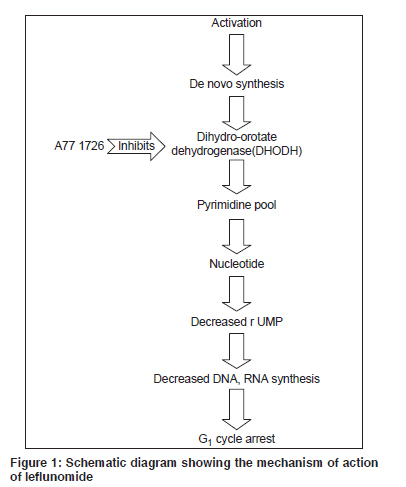
Activated lymphocytes require an eight-fold increase in ribonucleotide uridine monophosphate (rUMP) and other pyrimidine nucleotides to progress from G1 to S phase of cell cycle for proliferation and they must use the de novo pyrimidine synthesis. [1],[2] A77 1726 (active metabolite) inhibits dihydroorotate dehydrogenase , an enzyme involved in de novo pyrimidine synthesis. Inhibition of this enzyme leads to decreased rUMP, decreased DNA and RNA synthesis, inhibition of T-cell proliferation and G1 cycle arrest [Figure - 1].
The active metabolite also inhibits protein kinase activity and T-cell dependent B-cell formation of autoantibodies (IgG and IgA). [3]
Anti inflammatory action
A77 1726 interferes with T-cell production of inflammatory cytokines by preventing activation and gene expression of nuclear factor (NF) kB required for expression of inflammatory cytokines. [4] It also increases the production of immunosuppressive TGF-β protein and inhibits the production of proinflammatory TNF-α and interleukin 1β. [2],[4] A77 1726 has a direct effect on inhibition of COX-2 enzyme at the site of inflammation.[5]
Drug Interactions
Side effects may occur when leflunomide is given concomitantly with hepatotoxic agents. This point also should be considered when leflunomide treatment is followed by drugs without a drug-elimination procedure, e.g. methotrexate. [6] The active metabolite of leflunomide, i.e. A77 1726 persists in the blood for two years after drug cessation, hence side effects may continue to develop several weeks after the drug is stopped. The resulting concomitant hepatotoxicity could be due to persistence of this active metabolite and simultaneous administration of methotrexate.
Administration of cholestyramine or active charcoal causes decreased levels of active metabolite. This interaction is used in drug washout procedure in cases of serious adverse effects or reproductive issues (discussed in later section). [7]
The concomitant or sequential use (without the recommended leflunomide washout period or procedure) of oral retinoids, e.g. acetretin, NSAIDs known to induce hepatotoxicity may potentiate the risk of liver injury associated with leflunomide. Following concomitant administration of a single dose of leflunomide to patients receiving multiple doses of rifampin, A77 1726 peak levels are increased.[7] Leflunomide is a weak inhibitor of cytochrome P450. The co-administration of leflunomide with tolbutamide causes an increase in tissue concentration of tolbutamide and hence should be avoided.
Contraindications Leflunomide is contraindicated in the following patient groups:
- Patients with known hypersensitivity to drug. [7]
- Pregnant women or women of child-bearing age group not using reliable contraceptive method. Women on treatment should not become pregnant before 2 years of completion of therapy. [8]
- Patients with pre-existing liver or renal disease. [9]
- Patients with severe immunodeficiency or bone marrow dysplasia.
- Active infections (Bacterial, viral or fungal).
- Avoided in combination with hepatotoxic drugs such as methotrexate, acetretin, NSAIDs and alcohol.
Indications for Use
- Rheumatoid arthritis [2],[7],[10]
- Psoriatic arthritis [2],[7],[15]
- SLE [11]
- Wegener′s granulomatosis [12]
- Crohn′s disease [13]
- Takayasu′s arteritis [14]
- Ankylosing spondylitis [14],[15]
- Sarcoidosis [16]
- Felty′s syndrome
- Bullous pemphigoid
- Polyoma BK virus nephropathy
- Juvenile rheumatoid arthritis (FDA Approval Pending)
Drug Monitoring
Table 1
Dosage of Leflunomide Leflunomide is available in tablets of 10, 20 and 100 mg. [7],[8],[10] Oral loading dose of 100 mg daily for 3 days is given to rapidly reach a steady drug level. The initial loading dose is followed by maintenance dose of:
- 10-20 mg daily for rheumatoid arthritis
- 20 mg daily for psoriatic arthritis
Total duration of treatment is from 1 to 2 years. [2]
Side Effects
- Most common side effect of leflunomide is diarrhea. Other gastro-intestinal side effects are colitis, cholelithiasis, esophagitis and aphthous stomatitis. [7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17]
- Liver toxicity - Most cases of liver toxicity are seen within 6 months of treatment when multiple risk factors are present (hepatotoxin, previous liver diseases). Manifestation of liver toxicity ranges from mild jaundice to severe permanent hepatitis, severe liver necrosis and liver cirrhosis.
- Myelosuppression - Anemia, leukopenia and thrombocytopenia.
- Skin - Life-threatening Stevens Johnson syndrome or Toxic epidermal necrolysis, acne eruptions, hair discoloration, alopecia, maculopapular rash and nail discoloration seen in less than 1% patients.
- Respiratory infection with Pneumocystis jiroveci and aspergillus which manifests as non-reversible asthma and dyspnea.
- Others - Other side effects are CVS (angina, palpitation), CNS (anxiety, depression and insomnia). Few cases of anaphylaxis have also been reported.
Leflunomide Elimination and Washout This is recommended to achieve nondetectable plasma levels of leflunomide after stopping treatment. [7],[8] The aim of washout procedure is to bring plasma level of leflunomide to less than 0.02 mg/l or 0.02µg/ml. The drug elimination procedure is indicated in:
- Female patients who plan to start a family
- Worsening of respiratory symptoms or onset of new symptoms
- Patients with renal insufficiency
- In cases of adverse cutaneous drug reactions to leflunomide
- Simultaneous administration of drugs with hepatotoxic potential
Procedure of drug washout
Cholestyramine 8 g three times daily for 11 days (The 11 days need not be consecutive unless urgent reduction of plasma level is needed). [17] Verification of plasma level of the drug should be done by two separate tests done 14 days apart. If the plasma level is more than 0.02 mg/L, additional cholestyramine treatment should be considered.
Administration of activated charcoal (powder made into a suspension) orally or via nasogastric tube 50 mg every 6 h for 24 h, in addition to the cholestyramine dose that can be given for rapid reduction of plasma levels.
In cases of cutaneous adverse reactions, leflunomide must be stopped. Depending on the severity, systemic steroids can be instituted along with other supportive measures. Oral cholestyramine 4 gm tid may be given as it is expected to help in the excretion of leflunomide by interfering with biliary secretion and reabsorption of leflunomide. [17]
Leflunomide has a beneficial effect when used in setting of nephrotoxicity; however, there are no controlled trials of leflunomide use in the setting of rheumatoid or psoriatic arthritis with nephrotoxicity. Physicians should use the drug with regular monitoring of renal parameters and stop the drug at the earliest sign of renal abnormality. [18]
References
| 1. | Breedveld FC, Dayer JM. Leflunomide: Mode of action in the treatment of rheumatoid arthritis. Ann Rheum Dis 2000;59:841-9. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Li EK, Tam LS, Tomlinson B. Leflunomide in the treatment of rheumatoid arthritis. Clin Ther 2004;26:447-59. Back to cited text no. 2 [PUBMED] [FULLTEXT] |
| 3. | Siemasko KF, Chong ASF, William JW, Bremer EG. Regulation of B cell function by the immunosuppressive agent leflunomide. Transplantation 1996;61:635-42. Back to cited text no. 3 |
| 4. | Manna K, Agarwal BB. Immunosuppressive leflunomide metabolite (A77 1726) blocks TNF-dependant nuclear factor-kappa B factor activation and gene expression. J Immunol 1999;162:2095-102. Back to cited text no. 4 |
| 5. | Hamilton LC, Vojnovic I, Marner TD. A77 1726, the active metabolite of leflunomide, directly inhibits the activity of cyclo-oxygenase-2 in vitro and in vivo in a substrate sensitive manner. Br J Pharmacol 1999;127:1589-96. Back to cited text no. 5 |
| 6. | Weinblatt ME, Kremer JM, Coblyn JS. Pharmacokinetics, safety and efficacy of combination treatment with methotrexate and leflunomide in patients with active rheumatoid arthritis. Arthritis Rheum 1999;42;1322-8. Back to cited text no. 6 |
| 7. | Kale VP, Bichile LS. Leflunomide: A novel disease modifying anti-rheumatic drug. J Postgrad Med 2004;50:154-7. Back to cited text no. 7 [PUBMED]  |
| 8. | Arava (leflunomide) Prescribing information as of September 2003. Aventis Pharmaceuticals Inc. Kansas City, MO 64137. Back to cited text no. 8 |
| 9. | Uppal M, Roy R, Srinivas CR. Leflunomide induced drug rash and hepatotoxicity. Indian J Dermatol 2004;49:154-5. Back to cited text no. 9 |
| 10. | Agarwal SK, Narsimulu G, Handa R. Leflunomide-The Indian Experience: A multicentre assessment of its safety and effectiveness in the treatment of active rheumatoid arthritis. J Indian Rheumatol Assoc 2002;10:30-5. Back to cited text no. 10 |
| 11. | Remer CF, Weisman MH, Wallace DJ. Benefits of leflunomide in systemic lupus erythematosus: A pilot observational study. Lupus 2000;10:480-3. Back to cited text no. 11 |
| 12. | Metzler C, Fink C, Lamprecht P. Maintainance of remission with leflunomide in Wegener's granulomatosis. Rheumatology (Oxford) 2004;43:315-20. Back to cited text no. 12 |
| 13. | Prajapati DN. Leflunomide treatment of Crohn's disease patient intolerant to Standard immunomodulator therapy. J Clin Gastroenterol 2003;37:125-8. Back to cited text no. 13 |
| 14. | Kiely PD. The broadening use of leflunomide in clinical practice. Hosp Med 2004;65:735-9. Back to cited text no. 14 [PUBMED] |
| 15. | Pham T, Fautrel B. Recommendations of the French Society for Rheumatology regarding TNF alpha antagonist therapy in patients with ankylosing spondylitis or psoriatic arthritis: 2007 update. Joint Bone Spine 2007;74:638-46. Back to cited text no. 15 |
| 16. | Baughman RP, Lower EE. Novel therapies for sarcoidosis. Semin Respir Crit Care Med 2007;28:128-3. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Veeranna S, Jayadev B, Kushalappa PA. Severe cutaneous adverse drug reaction to leflunomide: A report of 5 cases. Indian J Dermatol Venereol Leprol 2006;72:286-9. Back to cited text no. 17 |
| 18. | Hardinger KL, Wang CD, Schnitzler MA. Prospective, pilot, open-label, short-term study of conversion to leflunomide reverses chronic renal allograft dysfunction. Am J Transplant 2002;2:867-71. Back to cited text no. 18 |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09139t1.jpg]
[dv09139f1.jpg]
|

{kind=link}
{kind=link}