
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 75, Num. 4, 2009, pp. 425-434
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 425-434
Residents Corner
Sutures and suturing techniques in skin closure
Kudur MohanH, Pai SathishB, Sripathi H, Prabhu Smitha
Department of Dermatology, Kasturba Medical College, Manipal - 576 104, Udupi Dist, Karnataka
Correspondence Address:Dr. Mohan H Kudur, Department of Dermatology, Kasturba Medical College, Manipal - 576 104, Udupi Dist, Karnataka
mohankudur@rediffmail.com
Code Number: dv09166
PMID: 19584482
DOI: 10.4103/0378-6323.53155
Introduction Even today, there is a search for ideal suture material. Suture materials can be broadly classified as naturally occurring and synthetic. [1] They can be further classified as monofilament or multifilament (braided), dyed or undyed, coated or uncoated. Several parameters, such as tensile strength, breaking strength, elasticity, capillarity and memory are used to describe physical characteristic of sutures. [2] In general, braided sutures are more prone to infection and induce greater degree of tissue reaction. Advantages of braided sutures include ease of handling, low memory and increased knot security. A monofilament suture is a single material. These sutures have decreased tendency of infection, ease of passage through tissue and ease of removal. They possess poor handling characteristics and decreased knot security.
Characteristics of an Ideal Suture Ideal suture material should:
- Have good handling characteristics
- Not induce significant tissue reaction
- Allow secure knots
- Have adequate tensile strength
- Not cut through tissue
- Be sterile
- Be non-electrolytic
- Be non-allergenic
- Cheap
Classification of Suture Materials
Absorbable
Natural: Catgut-plain or chromic
Synthetic: Polyglactin (vicryl), polyglycolic acid (dexon)
Non-absorbable
Natural: Silk linen
Synthetic: Polyamide (nylon), polyester (dacron), polypropylene (prolene)
Basic Characteristics of Wound Healing After Suturing A surgical wound never attains the same cutaneous tensile strength as of normal uncut skin. Two weeks after suturing, 3-5% of original strength will be achieved by a surgical wound. By the end of third week, 20% of the ultimate wound strength is achieved, and by one month only 50% of wound strength is attained. All sutures are foreign bodies and produce an inflammatory response in the host dermis. Peak inflammatory response is seen between second and seventh day with abundance of polymorphonuclear leukocytes, lymphocytes, and large monocytes in dermis. [3] Between the third and eighth day, the epithelial cells deeply invade the suture tracts.
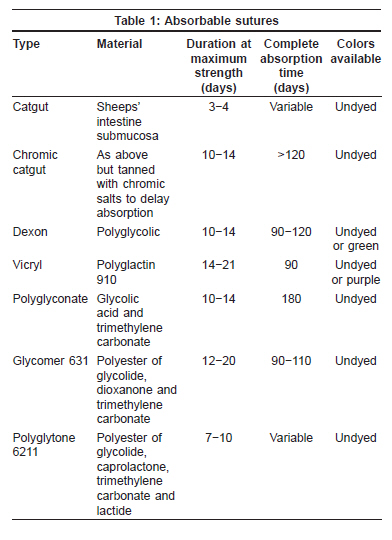
Absorbable Sutures
Absorbable sutures[4],[5],[6][Table - 1] are placed into subcutaneous tissue to eliminate dead space and into the dermis to minimize tension during wound healing.[4] Absorbable sutures must be placed well into dermis and subcutaneous tissue to facilitate this subsequent absorption by inflammation, enzymatic degradation or hydrolysis. If absorbable sutures are placed too superficially, they may persist for a prolonged period of time and thus possess an increased tendency to be transepidermally eliminated from the wound. This can compromise the appearance of the scar. Absorbable sutures are not intended to be used too close to the skin surface. This slows absorption and increases the likelihood of epithelization of the suture tunnels. This epithelization can result in permanent suture tracts and cyst formation.
Surgical gut
These sutures are derived from naturally occurring purified connective tissue (mostly collagen) of the small intestine of sheep or cattle. Surgical gut [4] is absorbed by proteolytic enzymatic degradation. Manufacturing may produce weak spots. This may cause uneven absorption of suture and its premature rupture. In comparison with the other absorbable sutures, surgical gut sutures tend to lose their strength rapidly. For this reason it is not wise to use this suture in patients predisposed to delayed wound healing. [5] Approximately 60% of the tensile strength of surgical gut is lost in a week and no tensile remains in two weeks. By treating with chromic salts, we can retard the absorption of surgical gut.
Polyglycolic acid (Dexon)
This is an absorbable braided synthetic homopolymer of glycolic acid. It is supplied as an uncoated or coated form. Coated polyglycolic acid [4],[5],[6] suture is undyed or dyed green, violet or bicolored. Since polyglycolic acid is not a naturally occurring organic substance, it elicits less inflammatory response than surgical gut. It is absorbed by hydrolysis. Polyglycolic acid possesses good tensile strength and excellent knot security. After two weeks of implantation, 65% of the initial tensile strength remains with polyglycolic acid suture, in contrast to 0% of surgical gut suture.
Polyglactin 910 (vicryl)
It is a synthetic heteropolymer consisting of 90% of glycolide and 10% of lactide. These sutures are braided, multifilament, coated, absorbable synthetic sutures. This suture is degraded by hydrolysis. This suture can be supplied in an antibiotic form by impregnating with triclosan. The residual tensile strength of a polyglactin 910 [4] suture is consistently greater than that of polyglycolic acid suture. Polyglactin 910 sutures are absorbed more rapidly than polyglycolic acid suture. In one study comparing the absorption of polyglactin 910 and polyglycolic acid, the absorption of former began approximately at 40 days, and was nearly complete by day 70. At 90 days, no polymer remained in the tissue.
Polyglyconate
It came in to market in 1985. It is synthetic monofilament absorbable suture, composed of glycolic acid and trimethylene carbonate. Polyglyconate [6] has some advantages over other sutures, such as improved handling properties, lacks memory, passes easily through tissues and demonstrates superior strength. It retains 75% of original strength at two weeks of postimplantation. Absorption is essentially complete by 180 days.
Glycomer 631
It is a synthetic absorbable monofilament suture, composed of polyester of glycolide (60%), dioxanone (14%) and trimethylene carbonate (26%). It has high flexibility, low memory and minimal tissue reactivity. It is degraded by hydrolysis. It passes through the tissue more easily but knot security is inferior. Absorption of Glycomer 631 [3],[4] is complete between 90 and 110 days.
Polyglytone 6211
Polyglytone 6211 [4],[5] is a recently developed monofilament, absorbable, synthetic suture. It is polyester of glycolide, caprolactone, trimethylene carbonate and lactide. It is undyed and uncoated. It loses its tensile strength rapidly, mimicking surgical gut. Absorption occurs via hydrolysis. Knot strength decreases to 50−60% of original strength at five days postimplantation.
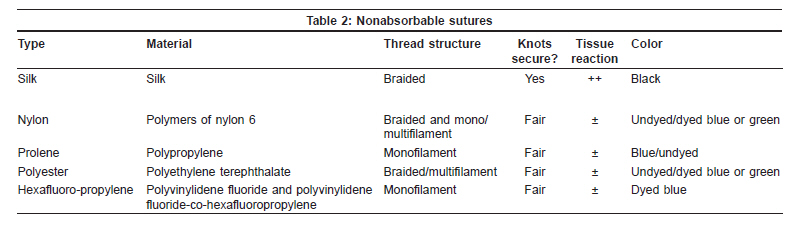
Nonabsorbable Sutures
Nonabsorbable sutures[4],[5],[6],[7],[8] [Table - 2] are more commonly used in dermatology and dermatosurgery than absorbable sutures. These sutures should be just tight enough to approximate, not strangulate tissues. [6] Nonabsorbable sutures may be used as deep sutures to provide prolonged mechanical support.
Silk
Surgical silk [6] is derived from silkworm species Bombyx mori of the family Bombycidae, the larva of which spins silk to weave its cocoon. It is a braided, black dyed, coated suture. Coating with wax or silicone helps to reduce tissue friction and capillarity. Silk is naturally occurring organic substance and induces a striking host inflammatory response. [7],[8]
A special quality of silk is its ease of handling. Unfortunately, its tensile strength is very low and it exhibits high capillarity, which increases the risk of infection. It loses approximately 50% of its strength in one year. Due to its property of reactivity, it is rarely used for cutaneous closures; however, it is commonly used on mucosal and intertriginous areas as it is soft and pliable.
Nylon
Nylon [5],[6],[7] suture materials are available in mono or multifilament forms. It is composed of long-chain aliphatic polymers of nylon 6. Due to its property of elasticity, it is useful for surface (epidermal, superficial) closure. Monofilament nylon suture has a great deal of memory (Memory is the ability of a suture material to return to previous shape after deformation.) and its proclivity for knot slippage is known. Multifilament braided nylon sutures exhibit decreased memory and they are associated with higher infection rate. In vivo , nylon loses 15−20% of tensile strength every year by hydrolyzation.
Polypropylene (Prolene)
Polypropylene (Prolene) [6],[7],[8] was devloped in 1970 as a first synthetic nonabsorbable suture. It is a monofilament suture. Prolene is made of isotactic crystalline stereoisomer of polypropylene with few unsaturated bonds. Polypropylene has a tensile strength more than nylon. It can easily pass through tissues and induces minimal host response. It does not adhere to the tissues and can be used as an intradermal suture. It is available as dyed or undyed form. It has good plasticity and it expands with tissue swelling to accommodate the wound. High memory, poor knot security and lack of elasticity are the few disadvantages with Prolene.
Polyester
Polyester [7],[8] sutures are nonabsorbable synthetic-braided multifilament sutures composed of polyethy-lene terephthalate. They are used for prosthetic implantations, face lifts and cardiovascular surgeries due to its unique properties, such as minimal tissue reactivity, high tensile strength, good handling and everlasting. It can be coated or uncoated.
Hexafluoropropylene
It is a newly developed monofilament suture made of polyvinylidene fluoride and polyvinylidene fluoride-co-hexafluoropropylene. [6] It exhibits lack of adherence to tissues which makes it a possible choice for ′pull- out′ sutures. Like polypropylene, it resists infection and elicits minimal tissue response. It is dyed blue. It is nonabsorbable and does not weaken after implantation.
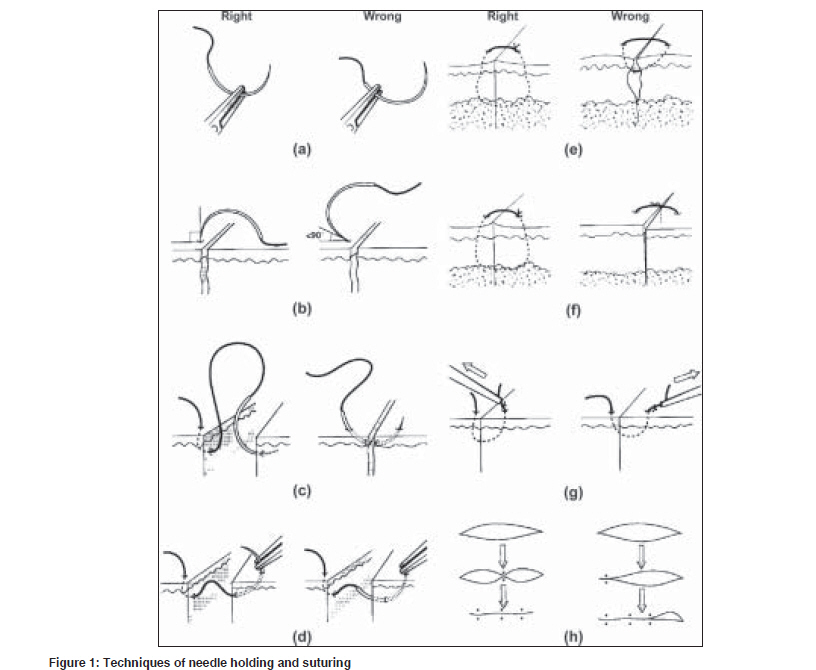
Needles
Suture needles [9],[10] should be handled carefully. Avoid blunting the cutting point or bending the weaker end of the suture needle. The needle should only be grasped with needle-holders in the middle third [Figure - 1]. Needles vary in size, shape and cross-section. [2],[9],[10]
Size
The aim is to use the thinnest needle and the finest filament the wound tolerates. Size of the suture material determines the thickness the suture needle being used. Different needle lengths are available for each suture size and the length required depends on the thickness of the tissue being sutured. The needle must be passed through the tissue at 90° to the skin surface and be long enough to be passed through the skin and then grasped by the forceps without damaging the tip [Figure - 1]. If the needle starts to bend during suturing and has to be bent back into shape then there is a risk that it will break. Loss of piece of needle in the wound might complicate an otherwise simple procedure.
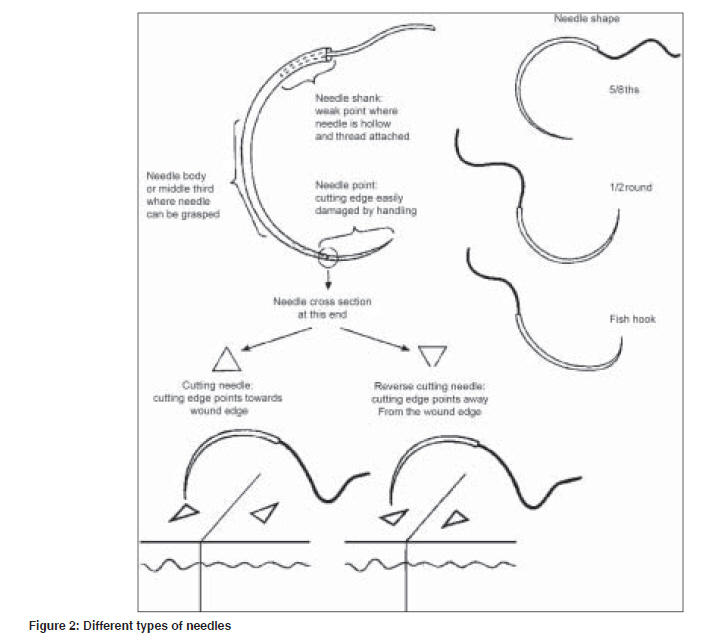
Shape
Curved needles are exclusively used in skin surgery. The curve may be three-eighths, half or five-eighths of a circle. It is shaped like a fish hook in case of subcutaneous sutures. It is important to rotate the wrist when passing the curved needle through the tissue [Figure - 2]. Simply pushing the needle into the tissue can break the needle.
Cross-section
Needles may be either cutting or non-cutting (round- bodied); the latter are not used in skin closure. Cutting needles may have their pointed or cutting edge on the inner or outer curve of the needle (i.e. a reverse-cutting needle). The cutting needle has the disadvantage that the cutting edge points towards the wound so that when the suture is pulled centrally, the suture material is more likely to tear through the skin. By contrast, there is less risk of suture material tearing through the wound edge when reverse-cutting needle is used [Figure - 2].
Suturing Techniques
Good suturing technique [9],[10] should eliminate dead space in subcutaneous tissues, minimize tension that causes wound separation. It involves correct wound placement with respect to relaxed tension lines. Other factors, such as systemic diseases and selection of suture material also influence the outcome. The surgical technique used to close a given wound depends on the force and direction of tensions on the wound, the thickness of the tissues to be opposed and anatomic considerations (e.g. eyes, vermilion border of the lips). [11],[12]
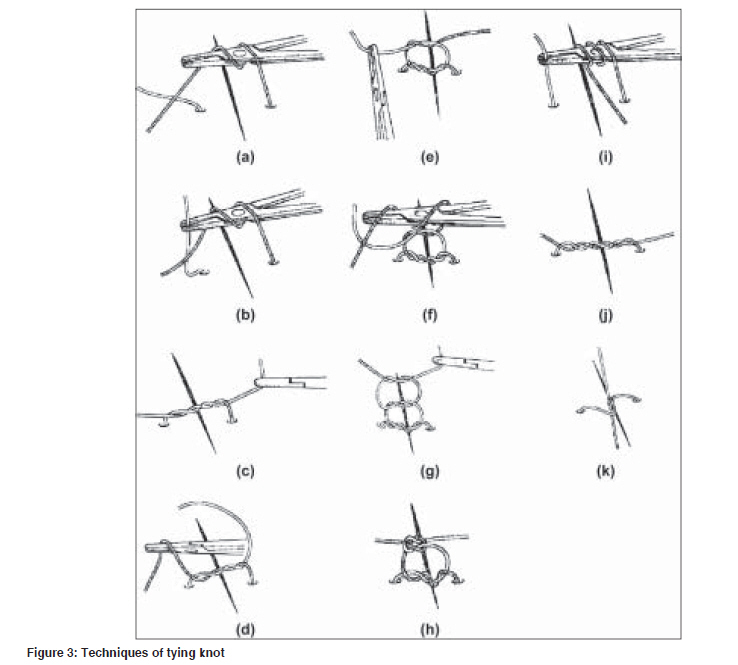
Knot tying
It is important to tie square knots when using monofilament nylon sutures because of the risk of knots unraveling spontaneously. [9],[11] If the knot starts to slip after the first two throws, since this increases the frictional force required to unravel the knot, or kink the knot by pulling the suture ends in the direction of rather than at right angles to the wound [Figure - 3].
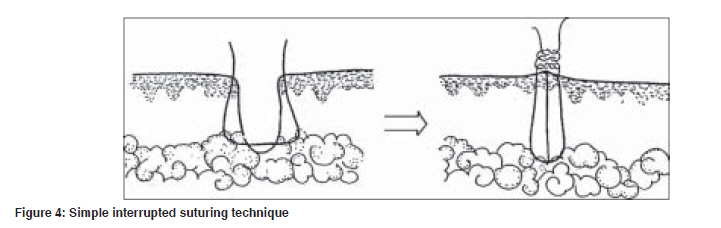
Simple interrupted suture
It is the most fundamental technique of wound closure used in cutaneous surgery.
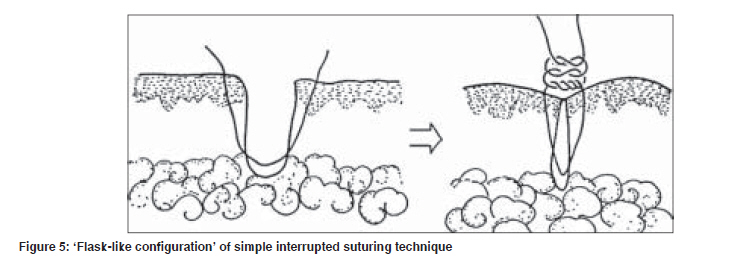
Procedure: To place a simple interrupted suture, [10],[11],[12],[13] the needle enters one side of the wound and penetrates well into the dermis or subcutaneous tissue. By altering the depth or angle of the needle, one can use this technique for wound edges of uneven thickness. The needle is then passed through the subcutaneous tissue to the opposing side of the wound and exists closer to the wound edge so that the final configuration of the suture is flask-shaped [Figure - 4]. The major disadvantage of this technique is that they tend to leave a series of crosshatched linear scars resembling railroad tracks. [13] Interrupted sutures tend to cause wound inversion if they are not placed correctly which can prevented by placing the suture in the flask-like configuration [Figure - 5].
Uses: Interrupted sutures are easy to place, possess greater tensile strength and have less potential to cause wound edema and impaired circulation.
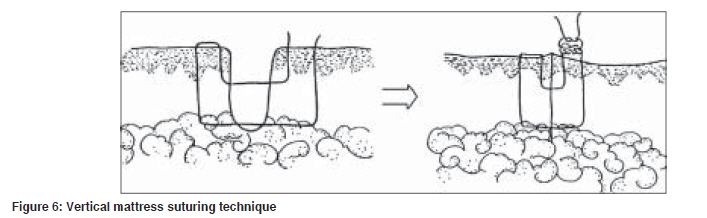
Vertical mattress suture
This is one of the best available suturing techniques to ensure eversion of wound and minimize significant wound tension.
Procedure: The vertical mattress suture [10],[11],[12],[13] is started 0.5-1cm lateral to the wound margin. Needle is inserted to the depth of the wound to close the dead space [Figure - 6]. The needle is then passed to the deep tissue to the opposing wound edge, where it exits the skin on the opposing side equidistant to the insertion. The needle is then reversed in the needle holder and the skin is penetrated again on the side through which the suture just exited but closer to the wound edge. It is passed more superficially to the opposite side, exiting close to the wound margin (1-3mm of wound margin).
This procedure is time-consuming. Improper technique causes wound inversion, uneven tension and increasing scarring. [13]
Uses: Useful in maximizing the wound eversion, reducing dead space and minimizing tension across the wound.
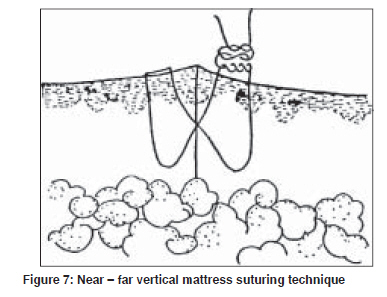
Near−far vertical mattress suture
This is a modification of standard vertical mattress suture [Figure - 7]. [13]
Procedure: Begin near the wound edge (1-3 mm), passing needle into the deeper aspect of the opposing side and exit through the epidermis wide to the insertion (0.5-1.0 cm). Reverse the needle and reenter the skin near the wound edge (1-3mm) of the side just exited and repeat the same procedure exiting wide to the initial penetration (0.5-1.0cm). This technique helps to elevate the deeper tissues of the wound and evert the epidermis.
Uses: It is used when tissue expansion is desired and closure of wound which is under tension.
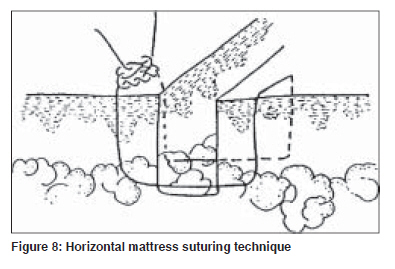
Horizontal mattress suture
Horizontal mattress suture [9],[10],[13] technique helps in minimizing the wound tension, closing the dead space and facilitating wound edge eversion.
Procedure: Penetrate the skin 5-10 mm from the edge of the wound [Figure - 8]. The needle is then passed dermally or subcutaneously toward the opposing wound edge where it enters at the same level in the subcutaneous or dermal tissue. Exit the opposing wound edge through the epidermis equidistant from the insertion. Reenter the skin on the same side at the same distance from the wound edge but several millimeters laterally. The needle is then passed dermally or subcutaneously to the side of initial penetration.
Horizontal mattress suture might cause strangulation of tissues leading to tissue hypoxia, necrosis and poor wound healing.
Uses: It is useful for wounds under high tension. This suture may also be used as a stay stitch to temporarily approximate wound edges. Horizontal mattress suture may be used prior to a proposed excision as a skin expansion technique to reduce tension.
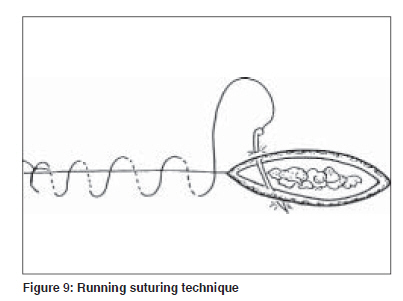
Running suture
Running suture [8],[10],[13] technique is useful over eyelids, ears and the dorsa of hands or can be used to secure the edges of a full-or split-thickness skin graft. The primary advantage of this technique is its relative ease and speed of placement.
Procedure: Initially place a simple interrupted suture at one end of a wound. This is tied but not cut. Simple sutures are placed down the length of the wound, re-penetrating the epidermis and passing dermally or subcutaneously [Figure - 9]. It is important to space each interval of the running suture evenly. The suture is terminated by placing a single knot between the suture materials as it exits the skin at the end of the incision.
Uses: Useful for long wounds in which wound tension has been minimized with properly placed deep sutures. It is also useful in securing a full-or split- thickness skin graft. Less chances of scarring when compared to interrupted sutures.
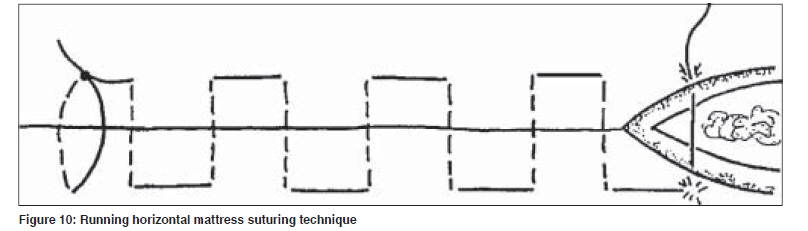
Running horizontal mattress suture
It is a modification of simple running suture. Instead of crossing over the wound prior to reentering the skin, the running horizontal mattress suture [13] is done by reentering the skin on the same side through which the suture material is exited [Figure - 10].
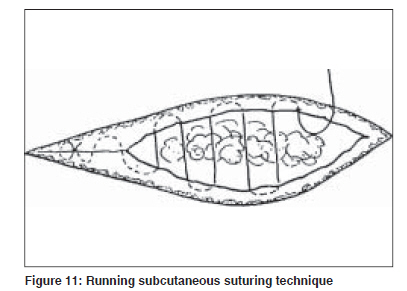
Running subcutaneous suture
The advantage of this technique is the relatively rapid speed with which it can be placed.
Procedure: It is initiated by placing a single subcutaneous suture [12] with the knot tied towards the wound surface. Then, it is looped through the subcutaneous tissue by passing through the opposite sides of the wound [Figure - 11]. It is tied at the distal aspect of the wound, with the terminal end of the suture to the previous loop placed on the opposing side of the wound.
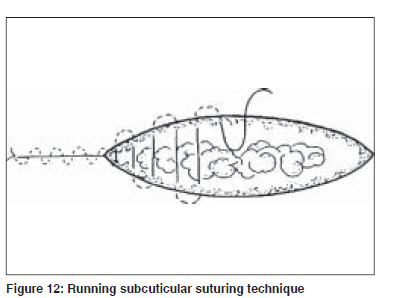
Running subcuticular suture
Running subcuticular suture [13] technique is useful to enhance the cosmetic result and is useful for closing wounds with equal tissue thickness and in which virtually no tension exists.
Procedure: It is initiated by placing a needle through one wound edge. The opposite edge is everted and the needle is placed horizontally through the upper dermis. This is repeated on alternating sides of the wound [Figure - 12]. The suture is terminated similarly to the running subcutaneous suture at the distal end of the wound. Absorbable subcuticular sutures may be used in children so that suture removal is avoided. [13] If the sutures are to be left for prolonged periods then nonabsorbable sutures such as nylon can be used.
Suture Removal Sutures should be removed at the earliest possible time to prevent or minimize suture reaction and suture marks but they should remain in place long enough to prevent wound dehiscence and scar spread. [9],[10] On the face and ears, sutures can be removed within 5-7 days, with eyelid sutures being removed in 3-5 days. Neck sutures are removed within 7 days and scalp sutures in 7-10 days. [12],[13] Sutures on trunk and extremities should be left in place for 10-14 days.Procedure
Suture line should be cleansed with an antiseptic. The interrupted suture is grasped with fine forceps at the knot and is cut on the side opposite the knot at the suture entry point into the skin. Next, the suture is gently pulled out by pulling toward the wound edge. A running suture is removed by cutting its every other loop and grasping the intervening loop with forceps and pulling it out. A running sub-cuticular suture is removed by cutting the knot at one end and pulling the suture out slowly from the other end to minimize the risk of suture breakage in the wound. [13]
Suture Material Selection When choosing a suture material, it is important to consider the location of wound, static and dynamic wound tension, presence of wound infection or fever and cost of suture material. If fever or chance of infection is high, then deep sutures composed of synthetic monofilament sutures are desirable, as braided sutures are associated with higher rates of infection and can be rapidly degraded by infection or fever. [14] For running intradermal sutures, polypropylene, poliglecaprone 25 or glycomer 631 can be considered. [14] They exhibit minimal tissue reactivity. For skin approximation, the smallest suture for the area should be used. For thin-skinned areas of low tension such as eyelids and scrotum 6-0 can be used; 5-0 is generally used for the face. For the facial areas closed under some tension, such as forehead and other body areas 4-0 can be used . [15] Thick skinned areas, such as scalp, back and scapular areas, closed under tension might require 3-0 or 2-0 to maintain the wound integrity. [16] Silk is best for approximation of mucosal and intertriginous areas. However, when the cosmetic appearance is important silk should not be used.
References
| 1. | Mackenzie D. The history of sutures. Med Hist 1973;17:158-68. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Swanson NA, Tromovitch TA. Suture materials. 1980: Properties, uses, and abuses. Int J Dermatol 1982;21:373-8. Back to cited text no. 2 |
| 3. | Postlethwait RW, Willigan DA, Ulin AW. Human tissue reaction to sutures. Ann Surg 1975;181:144-50. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Watts GT. Sutures for skin closure. Lancet 1975;1:581. Back to cited text no. 4 [PUBMED] |
| 5. | Moy RL, Lee A, Zalka A. Commonly used suture materials in skin surgery. Am Fam Physician 1991;44:2123-8. Back to cited text no. 5 [PUBMED] |
| 6. | Lober CW, Fenske NA. Suture materials for closing the skin and subcutaneous tissues. Aesthetic Plast Surg 1986;10:245-7. Back to cited text no. 6 [PUBMED] |
| 7. | Spelzini F, Konstantinovic ML, Guelinckx I, Verbist G, Verbeken E, De Ridder D, et al . Tensile strength and host response towards silk and type 1 polypropylene implants used for augmentation of Fascial repair in a rat model. Gynecol Obstet Invest 2007;63:155-62. Back to cited text no. 7 |
| 8. | Meinel L, Hofmann S, Karageorgiou V, Kirker-Head C, McCool J, Gronowicz G, et al . The inflammatory responses to silk films in vitro and in vivo . Biomaterials 2005;26:147-55. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Borges AF. Techniques of wound suture. Elective Incisions and Scar Revision. Boston: Little Brown 1973:65-76. Back to cited text no. 9 |
| 10. | Swanson NA. Basic Techniques. Atlas of Cutaneous Surgery. Boston: Little Brown 1987:26-49. Back to cited text no. 10 |
| 11. | Moy RL, Waldman B, Hein DW. A review of sutures and suturing techniques. J Dermatol Surg Oncol 1992;18:785-95. Back to cited text no. 11 [PUBMED] |
| 12. | Zachary CB. Suture techniques. In: Zachary CB, editor. Basic Cutaneous Surgery. New York: Churchill Livingstone 1991:53-75. Back to cited text no. 12 |
| 13. | Popkin GL, Robins P. Closure of skin wounds. Workshop Manual for Basic Dermatological Surgery. Kenilworth: NJ. Schering, Inc. 1983:18-36. Back to cited text no. 13 |
| 14. | Stegmen SJ. Suturing Techniques for dermatologic surgery. J Dermatol Surg Oncol 1978;4:63-8. Back to cited text no. 14 |
| 15. | Aston SJ. The choice of suture material for skin closure. J Dermatol Surg 1976;2:57-61. Back to cited text no. 15 [PUBMED] |
| 16. | Bennett RG. Selection of wound closure materials. J Am Acad Dermatol 1988; 18:619-37. Back to cited text no. 16 [PUBMED] |
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv09140t2.jpg]
[dv09140t1.jpg]
[dv09140f4.jpg]
[dv09140f11.jpg]
[dv09140f6.jpg]
[dv09140f12.jpg]
[dv09140f8.jpg]
[dv09140f7.jpg]
[dv09140f10.jpg]
[dv09140f2.jpg]
[dv09140f9.jpg]
[dv09140f3.jpg]
[dv09140f5.jpg]
[dv09140f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}