 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
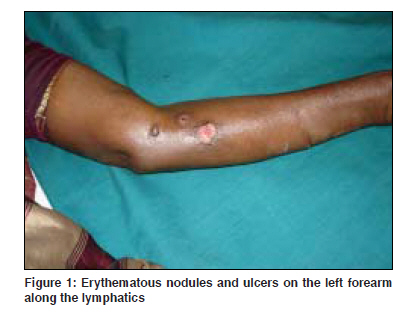
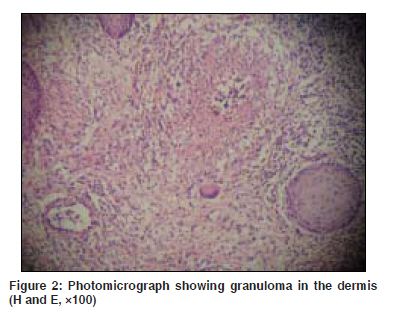
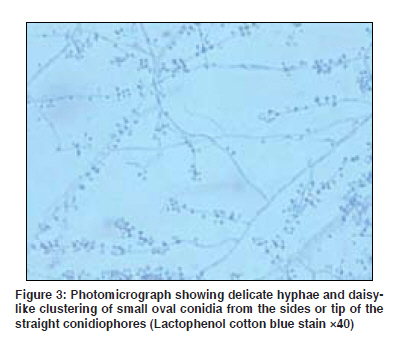
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 435-436 Quiz Linear nodules along the arm Martis Jacintha, Kamath GaneshH, Nandakishore B, Surendran K Department of Dermatology, Father Muller Medical College Hospital, Mangalore - 575 002, Karnataka Code Number: dv09167 PMID: 19584483 A 65-year-old female presented with painful reddish raised lesions over the left hand of 4 months duration following injury to the left middle finger. The skin lesions broke open to form an ulcer within a period of 2 months. Cutaneous examination revealed multiple discrete erythematous tender nodules of varying size over the normally appearing skin arranged in a linear pattern along the line of lymphatics extending upwards from the tip of the left middle finger to the lower part of the medial aspect of the left arm. A few lesions showed ulceration and crusting [Figure - 1]. There was no regional lymphadenopathy. Histopathological findings and lactophenol cotton blue stain findings are shown in [Figure - 2] and [Figure - 3]. What is your Diagnosis ? Diagnosis: Sporotrichosis Skin biopsy taken from the nodule under hematoxylin and eosin stain showed epidermal hyperkeratosis and granuloma in the dermis, consistent with the diagnosis of sporotrichosis [Figure - 2]. Fungal culture in Sabourauds agar from the nodule confirmed the diagnosis of sporotrichosis, showing the mycelial form of Sporothrix schenckii . Photomicrograph under lactophenol cotton blue stain showed the delicate hyphae and daisy-like clustering of small, oval conidia from the sides or the tips of straight conidiophores [Figure - 3]. Discussion Sporotrichosis is a subacute or chronic infection caused by the thermally dimorphic fungus S. schenckii , which is saprophytic in nature and is found throughout the world. [1] The disease occurs in temperate and tropical zones. It primarily involves the skin and subcutaneous tissue but dissemination may also occur. The mould is found on rose thorns, hay, spagnum moss, twigs and soil. Hence, the infection is more common among gardners. [2] Most of the reported cases are from Assam. A few cases have also been reported from Tamil Nadu, Karnataka, West Bengal and Himachal Pradesh. [3] In 1999, Ghosh et al. identified the hyperendemic area in Kangra district of Himachal Pradesh. [4] Hemashettar et al. reported a new endemic focus of sporotrichosis in northern Karnataka and southern Maharashtra. [5] Therefore, in India, at present, there are at least three recognised endemic zones representing the northeastern, northern and southern states of the country. [6] Cutaneous forms are of the following two types:
Differential diagnosis for lymphocutaneous sporotrichosis includes atypical mycobacterial infections, cutaneous tuberculosis, cutaneous leishmaniasis and anthrax. [3] Infection due to Mycobacterium marinum may closely resemble lymphangitic sporotrichosis. [7] Gummatous syphilis, bromoderma may mimic fixed cutaneous sporotrichosis. [3] Central nervous system involvement is more common in acquired immunodeficiency syndrome patients. [2] Periodic acid Schiff staining shows round to cigar-shaped yeast cells that have single or multiple buds. [8] Saturated solution of potassium iodide with milk or fruit juice is the standard treatment and should be continued for 3-4 days after clinical cure in systemic cases. [2] This patient was treated with oral gatifloxacin 400 mg once daily for 1 week. Saturated solution of potassium iodide five drops three times a day in one glass of milk was given initially and then gradually increased by 5 drops every week. The lesions regressed with the treatment. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09141f1.jpg] [dv09141f3.jpg] [dv09141f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}