 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
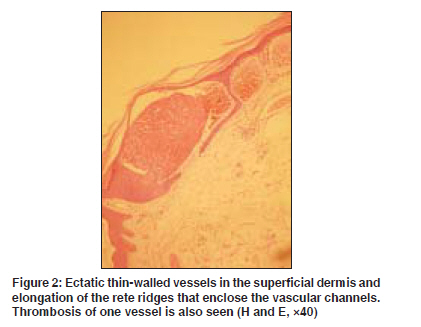
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 437 Net letter Multiple angiokeratomas on the breast Karadag AyseSerap, Simsek GulcinGuler Departments of Dermatology, Ankara Kecioren Research and Training Hospital, Ankara Code Number: dv09168 PMID: 19584485 Sir, Angiokeratomas are characterized by red to blue papules and consist of dilated dermal vessels with an overlying acanthotic epidermis. [1] There are five clinical types but other atypical forms have also been described. [1],[2] To the best of knowledge, angiokeratomas localized on the breast have not been reported till now in the literature. Our patient had multiple angiokeratomas on the breast skin, some of which were successfully treated with cryotherapy. A 43-year-old woman came with multiple lesions, approximately 1-4 mm in diameter over the left breast. They were red-blue, warty and non warty papules [Figure - 1]. There was no history of preceding trauma. She delivered a baby 7 years ago and these lesions initially appeared during the breast-feeding time. There was no size or shape difference between the two breasts. Dermatological examination of other areas was normal. General physical examination was normal. Breast ultrasonography was also normal. Histopathological examination of the representative lesion from the breast revealed hyperkeratosis and acanthosis with rete ridges wrapping up ectatic thin-walled dermal vessels and there was thrombosis in one of the vessels [Figure - 2]. The diagnosis of angiokeratoma circumscriptum naeviforme (ACN) was thus confirmed and treatment was initiated with cryotherapy for some of the lesions. Following treatment, there was only residual post inflammatory hyperpigmentation with some excoriations at the end of 1 month of follow-up [Figure - 3]. Angiokeratomas are well-circumscribed vascular lesions that are composed of superficial vascular ectasia with overlying hyperkeratosis. The clinical course, localization, gender distribution and age of onset vary widely between different types of angiokeratomas.[3] There are five distinct angiokeratoma types: ACN, angiokeratoma of Mibelli, angiokeratoma of Fordyce, angiokeratoma corporis diffusum (ACD) and solitary angiokeratoma. [1],[2] ACN is an unusual type of localized angiokeratoma that occurs most frequently in childhood and is usually characterized by large, linear and hyperkeratotic plaques. ACN is sometimes associated with an underlying vascular malformation and/or with atrophy or hypertrophy of the regional soft tissue and bone. [1],[3] Nevoid malformations or malformations of the underlying deeper vasculature might be a cause of ACN. Post traumatic arteriovenous fistula might be another cause of this type of angiokeratoma. Classic neviforme may not be seen in every case. The differentiation of ACN from verrucous hemangioma is sometimes challenging. [3] Angiokeratoma of Mibelli typically appears in young women on the dorsa of fingers and/or toes and presents with 1-5 mm diameter, multiple dark red papules. [3],[4] Atypical localizations include elbow, knee, shoulder and ear lobe. The lesion is usually preceded by a long history of recurrent chilblains and acrocyanosis. [3] Fordyce angiokeratomas are asymptomatic, 2-5 mm in diameter, blue-to-red papules localized on the scrotum, shaft of penis, labia majora or lower abdomen. They are usually associated with severe varicosity or varicocele.[3] ACD is typically characterized by innumerable small red to black papules occurring in clusters and is located symmetrically on the trunk.[3] ACD is an X-linked inherited disorder caused by a deficiency of the lysosomal enzyme alfa-galactosidase.[3],[5] Additionally, several patients without detectable abnormalities have been reported. [5] Solitary angiokeratomas are the most common form of angiokeratomas and the reported frequency varies from 70 to 83% of all angiokeratomas. [3] The lesions are thought to result from injury, trauma or chronic irritation of the wall of the venules in the papillary dermis. [1] They occur most commonly in the lower extremities. [2] The most common differential diagnosis involves melanocytic nevi, Spitz nevi, malignant melanomas, pigmented basal cell carcinomas, seborrheic keratoses, hemangioma and pyogenic granulomas. [2] Angiokeratoma can be treated with electrocautery, fulguration, CO 2 laser ablation, long-pulse vascular laser therapy or cryotherapy. [1],[3] The lesions in our patient were similar to ACN but our patient′s lesions had initiated during adulthood without underlying pathology. The breast-feeding might be the cause of local injury to the wall of a venule in the papillary dermis. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09142f3.jpg] [dv09142f1.jpg] [dv09142f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}