 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
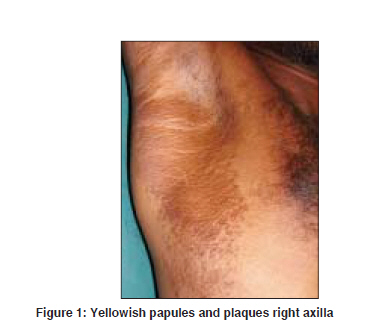
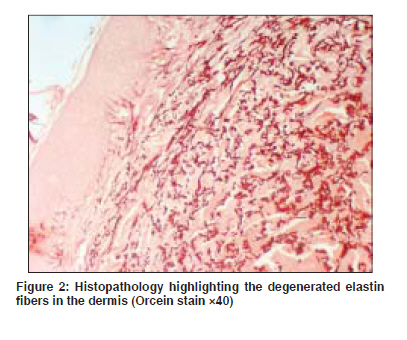
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 4, July-August, 2009, pp. 437 Net Quiz Asymptomatic yellowish papules and plaques over flexures Kaliyadan Feroze, Dharmaratnam AD, Jayasree MG, Parmar Chirag Department of Dermatology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala Code Number: dv09169 PMID: 19584484 A 27-year-old male patient presented to us with progressively increasing asymptomatic-raised skin lesions mainly over both axillae and groins since the age of 4 years. Since then, the area of involvement had increased slowly over the last few years. The patient did not have any other significant systemic and ophthalmic problems. No family member had similar or any other significant/relevant disease. On examination, yellowish papules and plaques were seen mainly over both axillae, sides of chest, groins and medial aspect of thighs [Figure - 1]. There were similar lesions scattered over the neck, cubital and popliteal fossae. There were no mucus membrane lesions. Systemic examination was within normal limits. Ophthalmological and cardiac evaluation was done, which was also normal. Investigations including complete blood counts, stool and urine examination, calcium/phosphate levels were all within normal ranges. A skin biopsy was taken. The Orcein stained image is shown [Figure - 2]. What is your Diagnosis ? Diagnosis: Pseudoxanthoma elasticum Discussion Pseudoxanthoma elasticum (PXE) is a heritable disorder characterized by progressive mineralization and fragmentation of elastic fibers mainly in the skin, eye and the cardiovascular system. [1] The molecular defect responsible can be acquired as an autosomal dominant or recessive trait and has been mapped to a gene on chromosome 16p13.1, which codes for an ATP-binding cassette sub-family C member 6 transporter (otherwise called the ABCC6 gene). [2],[3] Clinically, patients with PXE usually present in childhood with asymptomatic yellowish papules in the flexural skin (giving a ′plucked chicken′ appearance). Progressive involvement may affect the whole skin, particularly the neck, axillae and groins. The diagnosis can be confirmed by histopathological evaluation, which characteristically shows fragmented and calcified elastin fibers in the dermis. Special stains like Orcein (elastin) and Von Kossa (calcium) can be used to highlight the histological changes. The characteristic ocular defects are called ′Angioid streaks′, which result from the calcification of elastic fibers in the Bruch′s membrane in the retina. Cardiovascular involvement occurs secondary to the calcification of the elastic media of blood vessels. Patients may present with intermittent claudication, hypertension, myocardial infarction and even cerebral vessel involvement. Gastrointestinal hemorrhage secondary to fragility of calcified submucosal vessels is another common complication. [1],[4],[5] There is, however, no specific treatment for PXE as such. Plastic surgery/collagen injections can be tried for cosmetically bothersome skin lesions. Regular follow- up and monitoring for cardiovascular, gastrointestinal and ophthalmological complications is essential. [1] The skin lesions are important as they may help in early diagnosis of the disease thus reducing the risk of potential ophthalmic or cardiovascular complications. Pseudoxanthoma elasticum can easily be differentiated from other condition by a combination of the clinical and histological features. The clinical differential diagnosis of the skin lesions of PXE include conditions mimicking the papular lesions of PXE like acquired pseudo-PXE related to hemoglobinopathy, skin aging (chronological and/or actinic), elastoma, Buschke-Ollendorff syndrome, pseudo-PXE related to D-penicillamine, papular elastorrhexis and elastosis perforans serpiginosa. Some other conditions might mimic the plaque like lesions or redundant skin associated with PXE. These include - elastoderma, anetoderma, cutis laxa, etc. [2] The histology of PXE is very typical. Histological differentiation may be required from some conditions which might show some histological features akin to PXE, such as elastofibroma, elastosis perforans serpiginosa, calcinosis cutis, necrobiotic xanthogranuloma and necrobiosis lipoidica. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09143f2.jpg] [dv09143f1.jpg] |
| |||||||||


{kind=link}
{kind=link}