 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
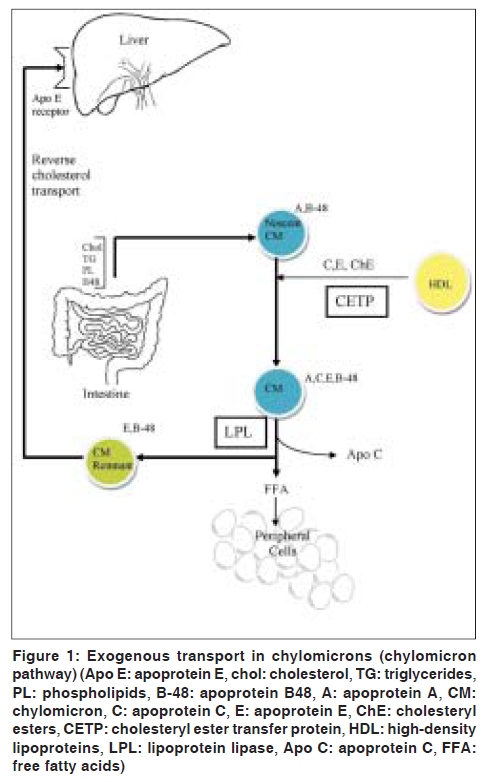
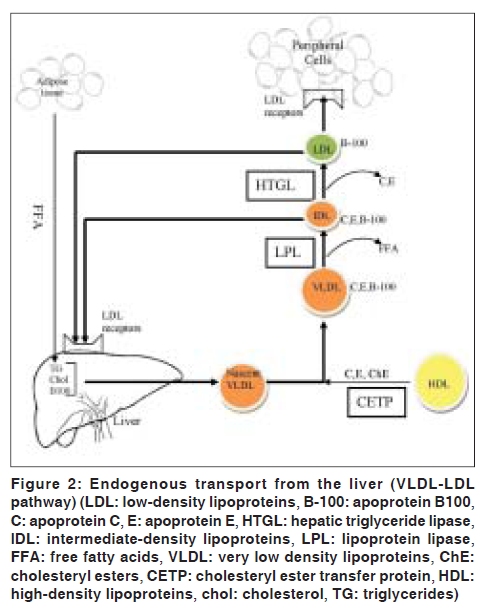
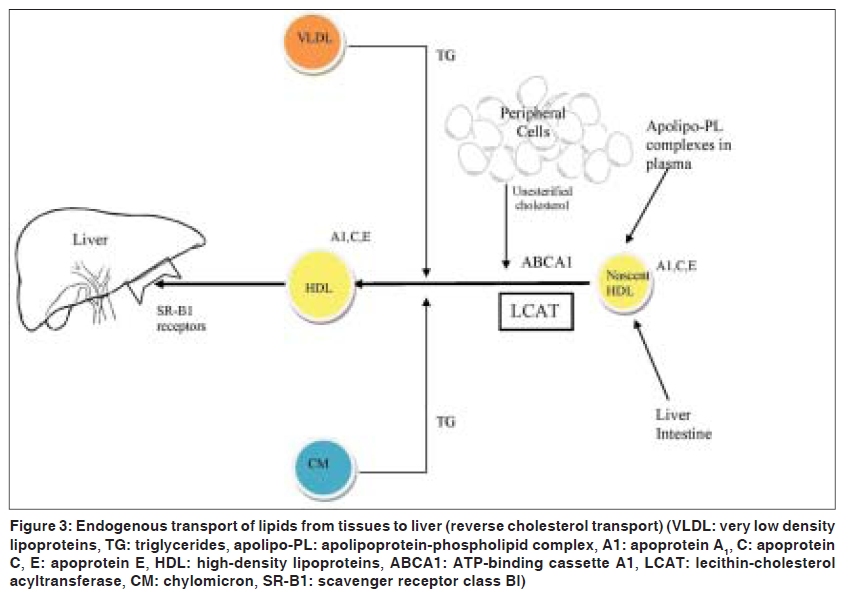
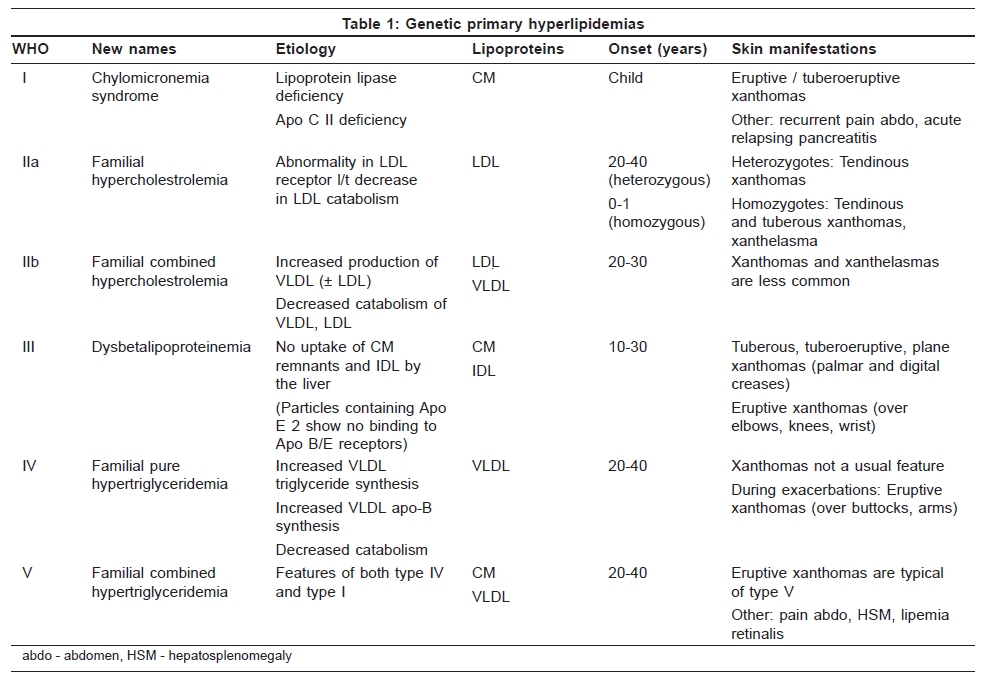
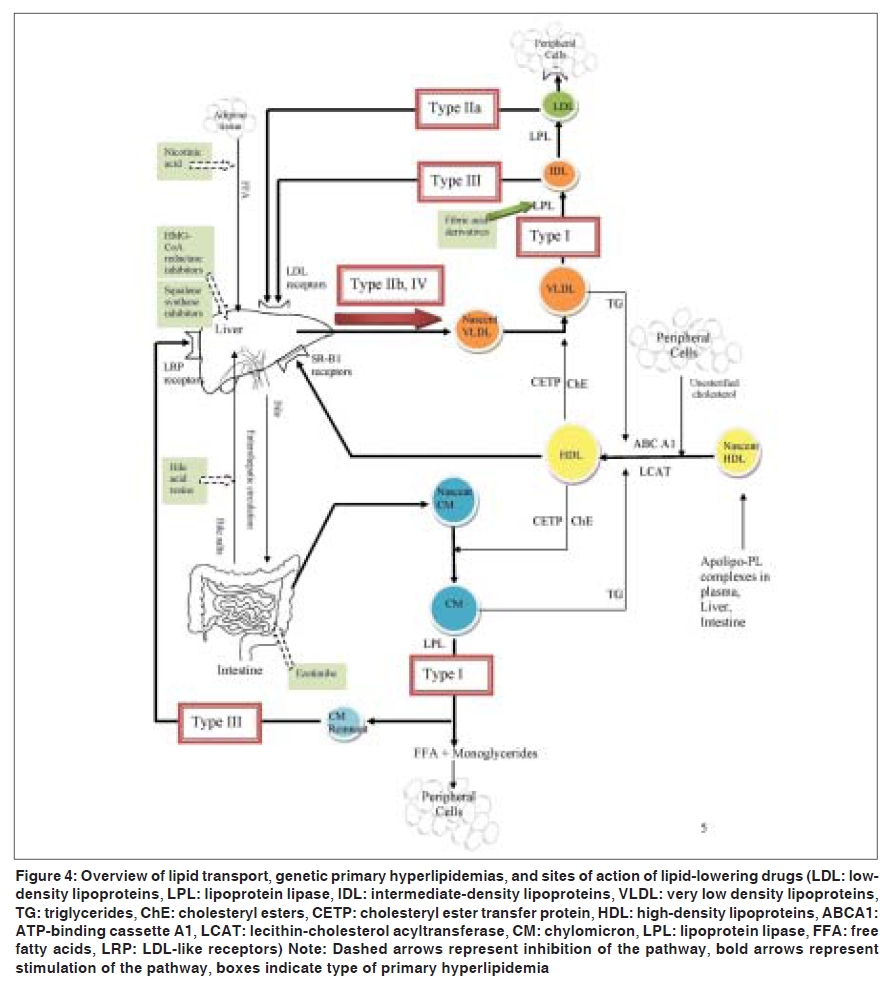
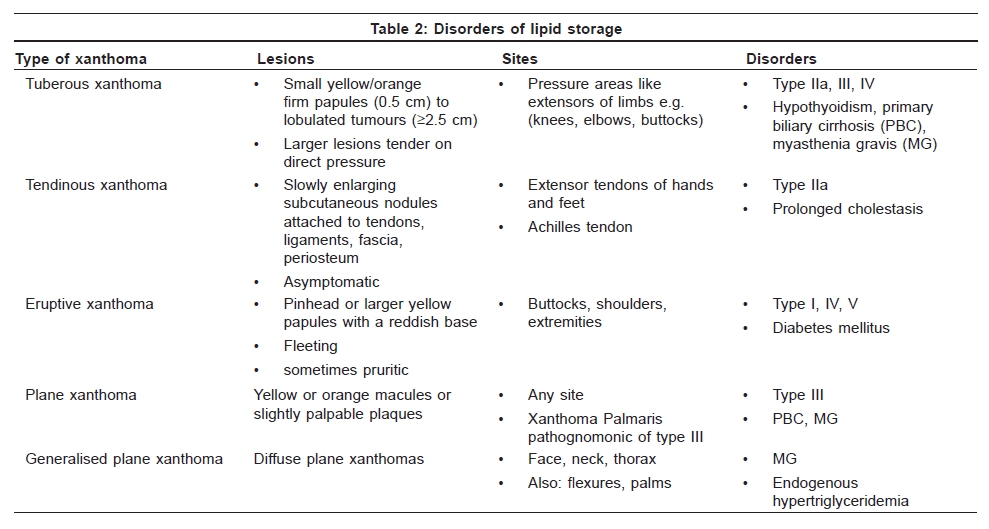
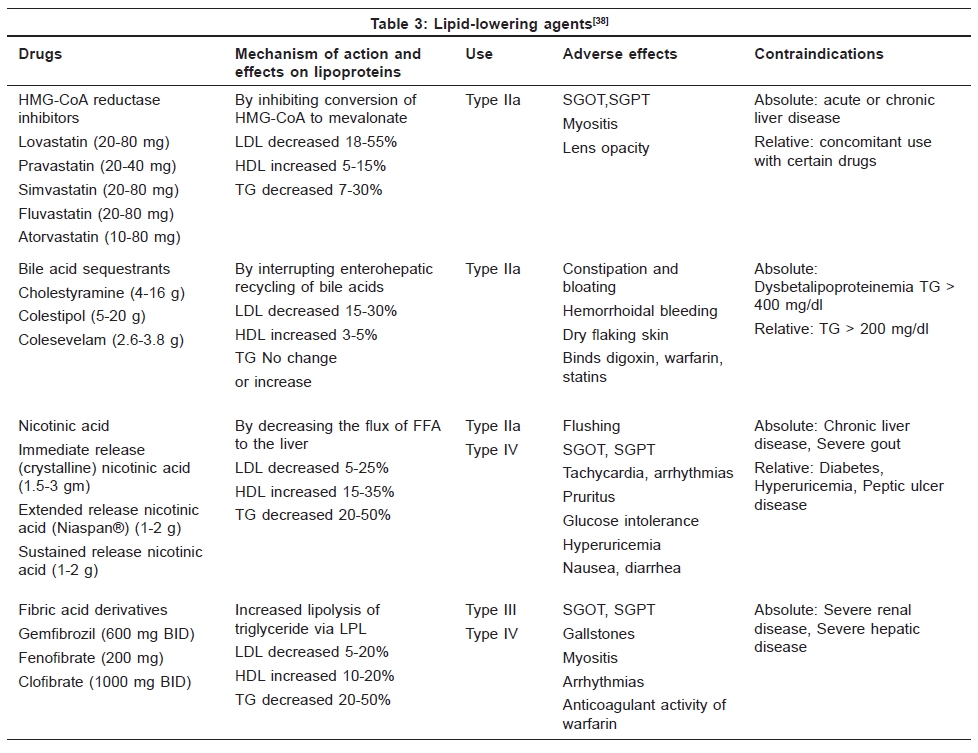
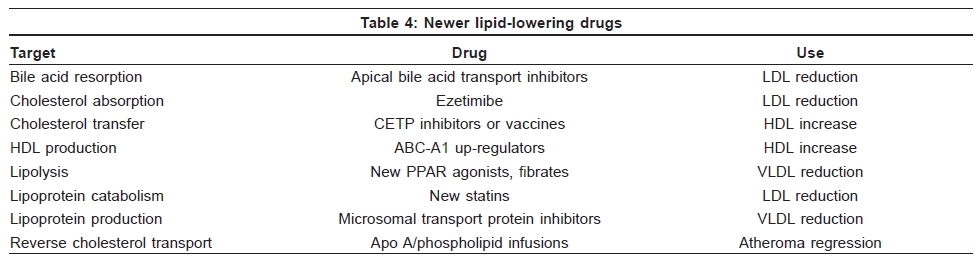
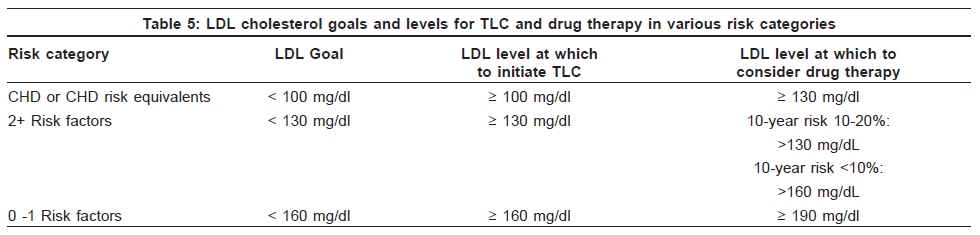
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 452-462 Review Article Management of hyperlipidemias: An update Nitin Ranjan Department of Dermatology, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, India Correspondence Address:Dr. Nitin Ranjan, Department of Dermatology, Jawaharlal Nehru Medical College, Aligarh Muslim University (AMU), Aligarh - 202 001, Uttar Pradesh, India Code Number: dv09149 PMID: 19736423 DOI: 10.4103/0378-6323.55387 Abstract The discovery of the key enzymes, receptors, and transporters in cholesterol biosynthesis has enabled us to assemble fragments of knowledge concerning lipids and lipoproteins into dynamic pathways, leading to the development of a multitude of lipid-lowering drugs. After a brief recapitulation of the pathways of cholesterol metabolism and the dermatologic manifestations of lipid derangement, we shall review drugs which modify intestinal cholesterol and bile-acid reabsorption, and hepatic lipoprotein biosynthesis and catabolism. The current literature is examined to determine future therapeutic targets in lipid metabolism, as well as the role of traditional foods as lipid-lowering agents. The latest National Cholesterol Education Program guidelines for managing hypercholesterolemia are also discussed.Keywords: Guidelines, Lipid metabolism, Low-density lipoprotein cholesterol, Statins Introduction Cholesterol serves not only as an essential component of the cell membrane but also as the precursor molecule from which steroid hormones, bile salts, and vitamin D are synthesized. It is both derived from the diet and synthesized within the body, mainly in the liver. Cholesterol circulates as a component of lipoproteins. The principal plasma lipoproteins are the chylomicrons (CMs), very low density lipoproteins (VLDL), low-density lipoproteins (LDL), and high-density lipoproteins (HDL). The principal fat in the diet is the triglycerides (TG), which are absorbed in the intestine. The lipoproteins are transported in combination with apoproteins (apo), like apo-A, apo-B, and apo-C. The Pathways Transport of lipoproteins can be divided into: Exogenous transport From ingested food to intestine to peripheral cells and liver [Figure - 1] Products of fat digestion from the gut (cholesterol, TG) are packaged with intestinal apo-B48 to form nascent CMs. This process is mediated by microsomal triglyceride transfer protein (MTP). [1] In the circulation, nascent CMs acquire cholesteryl esters (ChE), apo-C, and apo-E from HDL to form CMs. These CMs come in contact with lipoprotein lipase (LPL) located on the luminal surface of vascular endothelium of skeletal muscle and adipose tissue. LPL breaks down the triglyceride component of CMs into free fatty acids (FFA) and monoglycerides, in the process converting the CMs to smaller particles called CM remnants. The cholesterol-rich CM remnants are taken up by the liver via LDL-receptor-like-protein (LRP) receptors or Apo-E receptors. [2] In this way, dietary cholesterol finally reaches the liver. Endogenous transport From liver to peripheral tissues: the apo-B100 lipoprotein system [Figure - 2] Analogous to the secretion of nascent CMs by the gut, liver synthesizes and secretes nascent VLDL, by complexing TG and apo-B100 under the mediation of MTP. [1] Triglyceride-rich nascent VLDL serves as an efficient acceptor of ChE from HDL. This transfer takes place under the agency of cholesteryl ester transfer protein (CETP) in the plasma and leads to the formation of mature VLDL. [3] During circulation, LPL hydrolyses the TG of VLDL to FFA and monoglycerides, in the process converting VLDL to smaller lipoproteins called intermediate density lipoproteins (IDL), and further to still smaller ChE-rich LDL. LDL supplies tissues with cholesterol. Thus the liver serves as the major site for both cholesterol synthesis and LDL catabolism. From peripheral tissues to liver: the apo-A 1 lipoprotein system [Figure - 3] Nascent HDL particles are synthesized by apolipoprotein-phospholipid complexes in plasma, and also by intestine and the liver. Peripheral tissues (including liver) transfer unesterified cholesterol to nascent HDL by the membrane protein ATP-binding cassette protein A1 (ABCA1). [4] Lecithin-cholesterol acyltransferase (LCAT), an enzyme present on HDL, esterifies this cholesterol, leading to the formation of ChE. VLDL and CMs transfer TG to nascent HDL, which leads to formation of mature HDL. HDL is taken up directly by hepatocytes via the scavenger receptor class BI (SR-BI). [5] The transfer of excess cholesterol from the tissues back to the liver via HDL is called 'reverse cholesterol transport.' Hyperlipidemias Hyperlipidemias are classified as primary or secondary. Patients with primary hyperlipidemia have been classified into 5 major groups according to plasma lipoprotein patterns [Table - 1],[Figure - 4]. [6],[7] Conditions causing secondary hyperlipidemia include obstructive liver disease, various hematopoietic diseases (myeloma, Waldenstrom's macroglobulinemia, cryoglobulinemia, hemochromatosis), chronic renal failure, myxedema, pancreatitis, and drugs like estrogens, corticosteroids, and retinoids. [8] Dermatologic Markers of Lipid Derangement Abnormalities of lipid metabolism may favor lipid deposition in the skin and present as xanthomas. [9] Xanthelasma palpebrarum is the commonest type of cutaneous xanthoma and typically involves the upper eyelids as symmetrical, soft, yellowish papules and plaques near the medial canthi. [10],[11] The major lipid stored in xanthomas is esterified cholesterol. [12],[13] Xanthelasma is a marker of dyslipidemia, requiring a complete lipid profile to detect patients potentially at increased risk of cardiovascular disease. [14] However, only about half of the patients with xanthelasma are hyperlipidemic. [15] The most frequent hyperlipidemia associated with xanthelasma is type IIa. [16] Less frequently, types IIb, III, and IV are found. [16] Isolated xanthelasmata are often treated with destructive modalities, like trichloroacetic acid, electrocautery, surgical excision, [17] carbon dioxide laser, [18] pulsed dye laser, [19] and erbium:YAG laser. [20] A brief review of various other types of xanthomas is presented in [Table - 2]. Management Traditional foods and herbal therapies Dietary advice has a small but significant role to play in normalizing abnormal serum lipids in those at high risk of cardiovascular disease, and reductions in serum total cholesterol levels of the order of 3% to 6% are to be expected. [21],[22] Replacement of saturated fats by unsaturated fats leads to improved lipid levels.[23] However, it is not clear whether polyunsaturated or monounsaturated fats are most cardioprotective. [24] Rapeseed oil, which is rich in omega-3 fats, is especially useful. [25] Soluble fiber (in oats, pectin, psyllium, guar gum) results in a significant but very modest lipid-lowering effect.[26],[27],[28] Unrealistic (47g per day) intake of purified soy protein will lower total cholesterol levels by about 0.6 mmol L. [29] A recent review of the efficacy of garlic as an antihyperlipidemic agent found it difficult to recommend garlic as an antihyperlipidemic agent owing to the low methodological quality of the studies. [30] Stanol esters and plant sterols reduce cholesterol in those on an average diet, but may lack efficacy in those already on a low fat diet. [25] Drug treatment Statins One of the major advances in the management of hyperlipidemias has been the development of the statins, derived initially from fungi and later as purely synthetic molecules. [31],[32],[33] The statins are competitive inhibitors of 3-hydroxy-3-methyl-glutaryl-CoA (HMG-CoA) reductase, the rate-limiting enzyme in cholesterol biosynthesis. Inhibition of HMG-CoA reductase leads to a decrease in intrahepatic cholesterol concentration, to which the liver responds by inducing its LDL receptors, leading to an increase in receptor-mediated LDL catabolism. [32] Vis-à-vis the induction of LDL receptors, the SR-B1 receptors also increase their uptake of cholesterol from HDL. [34] However, the statins also decrease the activity of CETP. [35],[36] Thus the overall effect is a small increment in HDL. [34] Statins decrease serum triglycerides. [37] Statin-induced increased LDL-receptor activity also leads to the enhanced removal of the TG-rich lipoproteins VLDL and IDL. Similarly, increased activity of LDL receptor leads to enhanced uptake of CM remnants, thereby increasing postprandial TG clearance. Five statins are currently available [Table - 3]. [38] Out of these, rosuvastatin and atorvastatin are the most potent. [39] However, another response to statin-induced decrease in intrahepatic cholesterol is the increased expression of sterol regulatory element-binding proteins (SREBP). [40] This leads to increased synthesis of HMG-CoA reductase, essentially an attempt by the body at maintaining metabolic homeostasis. But this imposes a pharmacologic limitation on the amount of LDL lowering, which can be achieved by treatment with HMG-CoA reductase inhibitors. Development of noncompetitive inhibitors of HMG-CoA reductase, like apomine, is the solution. [41] Bile-acid sequestrating agents (BASA) BASA are anion exchange resins, which bind bile acids in the intestinal lumen. The physiological process of enterohepatic circulation involves reabsorption of bile acids in the terminal ileum and their circulation back to the liver. [42] BASA bind the bile acids, thus impeding their reabsorption and significantly increasing their fecal excretion. In response, the liver steps up the synthesis of bile acids from cholesterol. This leads to the depletion of intrahepatic cholesterol, which causes increased expression of LDL receptors. [43] Hepatic LDL uptake is thereby raised, and the net result is a decrease in LDL. BASA promote apo-A1 synthesis by an unknown mechanism and tend to raise HDL levels.[44] Three BASA are currently available [Table - 3]. Their use has been hindered by inconvenient dosing and by unpleasant side effects (e.g., constipation). [45] However, colesevelam appears to be better tolerated than the older resins. [46],[47] BASA nonspecifically bind anions and interfere with absorption of a number of drugs which are anionic at intestinal pH (statins, fenofibrate, corticosteroids, diuretics, tricyclic antidepressants, nonsteroidal anti-inflammatory drugs, thyroxine, and digoxin). These drugs should be administered at least 4 hours after or 1 hour before the last dose of BASA. [48] As BASA tend to raise triglycerides, they are contraindicated in patients with hypertriglyceridemia (>400 mg/dL). [49] Nicotinic acid (NA) Plasma FFA are immediate precursors of hepatic and subsequently plasma triglycerides transported in VLDL. NA is immediately taken up by adipose tissue via a specific high-affinity G-protein-coupled receptor. [50] It then inhibits lipolysis in adipose tissue, resulting in a decrease in plasma FFA. NA, in a dose-dependent way, lowers triglyceride-rich VLDL and cholesterol-rich LDL. [51] Furthermore, NA is the most potent HDL-raising drug. [52] But the unpleasant side effect of flushing precludes many patients from taking this drug. [53] Three formulations of NA are currently available [Table - 3]. Of these, the prolonged-release (PR) preparation, [54] also called extended-release (ER) preparation, has absorption rates between those of IR (immediate-release) and SR (sustained-release) preparations, and a lesser frequency and intensity of causing flush. [55] Fibric acid derivatives (fibrates) The lipid-modifying effects of fibrates are largely mediated by their ability to activate peroxisome proliferator-activated receptors (PPARs). [56] PPARs are ligand-activated transcription factors that control gene expression by interacting with response elements located upstream. PPARa is expressed primarily in the liver and brown adipose tissue. PPARa controls a number of genes involved in lipid metabolism, including those encoding for apo-CIII, apo-AI, and apo-AII. [57] Fibrates reduce triglycerides through PPARa-mediated reduced expression of apo-CIII, which serves as an inhibitor of lipolytic processing and receptor-mediated clearance. This leads to increased LPL synthesis and enhanced clearance of triglyceride-rich lipoproteins. Fibrate-mediated increases in HDL are due to PPARa stimulation of apo-AI and apo-AII expression. [58] Three fibric acid derivatives are currently available [Table - 3]. Fibrates are primarily used for lowering elevated triglycerides because the LDL cholesterol-lowering effects of fibrates are generally only 10% or less in persons with hypercholesterolemia. [38] Fenofibrate, however, reduces LDL cholesterol by a relatively greater extent than gemfibrozil. [59] Other therapeutic targets in lipid metabolism Guggulsterone (gugulipid) is a widely used yet controversial hypolipidemic drug. The plant sterols E- and Z-guggulsterone are the active compounds [60] derived from the gum resin of the mukul myrrh tree (Commiphora mukul). They act as antihyperlipidemic agents via the antagonism of the Farnesoid X receptor (FXR) [61],[62] and up-regulation of the bile salt export pump (BSEP). [63] E- and Z-guggulsterone are currently marketed under the brand name Gugulipid. Most of the clinical trials conducted in Asia demonstrated hypolipidemic activity of gugulipid with an average decrease of 10%-30% and 10%-20% in total cholesterol and triglyceride respectively. [63] However, the first and only clinical trial conducted in the U.S. population found that gugulipid did not improve the levels of serum cholesterol and might in fact raise LDL levels. [64] A recent review concluded that at present, there is not enough scientific evidence to support the use of guggul for any medical condition. [65] Larger clinical trials are required to obtain extensive clinical knowledge of this drug. A number of lipid-lowering pharmacological agents are currently under evaluation [Table - 4]. [66],[67] The most promising among these are ezetimibe [68] and squalene synthase inhibitors. [69] Ezetimibe blocks uptake of cholesterol into jejunal enterocytes, hence selectively blocking dietary and biliary cholesterol absorption from the gut. It acts by decreasing the intestinal cholesterol supply to the liver, lowering hepatic cholesterol levels and thus inducing LDL receptor expression. [70] Unlike the bile-acid sequestrants, it does not interfere with absorption of fat-soluble drugs. Moreover, ezetimibe does not increase serum TG. [71] Squalene synthase (SS) is the first enzyme in the hepatic cholesterol biosynthetic pathway which produces a metabolite (lanosterol) committed to cholesterol synthesis. [72] The result of inhibition of SS is analogous to that of HMG-CoA reductase. Induction of LDL receptors occurs, leading to a decrease in circulating LDL. Thus SS inhibitors act similar to statins, albeit at a different and a more specific level. [72] NCEP Guidelines The NCEP Adult Treatment Panel (ATP) first published guidelines for managing hypercholesterolemia in 1988 (ATP I) [73] and revised them in 1993 (ATP 2). The latest NCEP report (ATP III) has been published in 2001. [38] The first step is to determine lipoprotein levels after a 9- to 12-hour fast. [38] Next, coronary heart disease (CHD) risk equivalents and major risk factors should be established. CHD risk equivalents include clinical CHD, symptomatic carotid artery disease, peripheral arterial disease, abdominal aortic aneurysm, and diabetes. Major risk factors (exclusive of LDL cholesterol) include cigarette smoking, hypertension, low HDL cholesterol (< 40 mg/dL), family history of premature CHD, and age (men> 45 years; women> 55 years). CHD risk equivalents and risk factors are then used to determine the risk category of the patient [Table - 5]. Therapeutic lifestyle changes (TLC) [38] are considered first-line therapy in the management of high cholesterol. A 3-month trial of TLC should precede the use of drug therapy. The essential features of TLC are (a) reduced intake of saturated fats [less than 7% of total calories] and cholesterol [less than 200 mg/d]; (b) therapeutic options for enhancing LDL lowering - such as plant stanols/sterols [2 g/d] and increased soluble fiber [10-25 g/d; (c) weight reduction; and (d) increased physical activity. According to ATP III, the most cost-effective approach to prevention of CHD is: diet modification, exercise, and weight control, combined with avoidance or cessation of smoking. Cigarette smoking is a strong, independent risk factor for CHD and leads to elevated triglycerides and low HDL levels. Smoking cessation should receive prime emphasis in the clinical strategy to reduce CHD risk. While moderate intakes of alcohol in middle-aged and older adults may reduce risk for CHD, high intakes of alcohol produce multiple adverse effects. No more than 2 drinks per day for men and no more than 1 drink per day for women should be consumed. Persons who do not drink should not be encouraged to initiate regular alcohol consumption. Physical activity as a component of TLC includes enough moderate exercise to expend at least 200 kcal per day. Thus life-habit changes - weight control, exercise, and smoking cessation - will favorably modify multiple risk factors, including elevated triglycerides and low HDL levels. However, for patients with CHD or CHD risk equivalents and an LDL cholesterol level of 130 mg/dL or higher, an LDL-lowering drug may be started simultaneously with TLC to achieve the LDL goal of less than 100 mg/dL. The NCEP recommends the use of statins as first-line therapy when LDL cholesterol-lowering drugs are indicated. BASA's LDL-lowering effects may be enhanced in combination with other cholesterol-lowering medications, particularly statins. Nicotinic acid is recommended for high-risk patients with low levels of LDL cholesterol, high triglycerides, and low HDL cholesterol - a triad known as atherogenic dyslipidemia. [38] Fibrates are primarily used for persons with very high triglycerides to reduce risk for acute pancreatitis and for those with dysbetalipoproteinemia. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09149t5.jpg] [dv09149t1.jpg] [dv09149t4.jpg] [dv09149f3.jpg] [dv09149f2.jpg] [dv09149f4.jpg] [dv09149t2.jpg] [dv09149f1.jpg] [dv09149f5.jpg] [dv09149t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}