 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
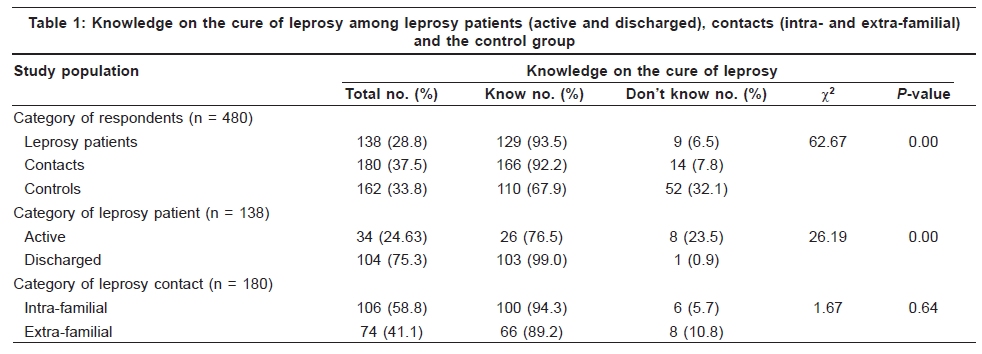
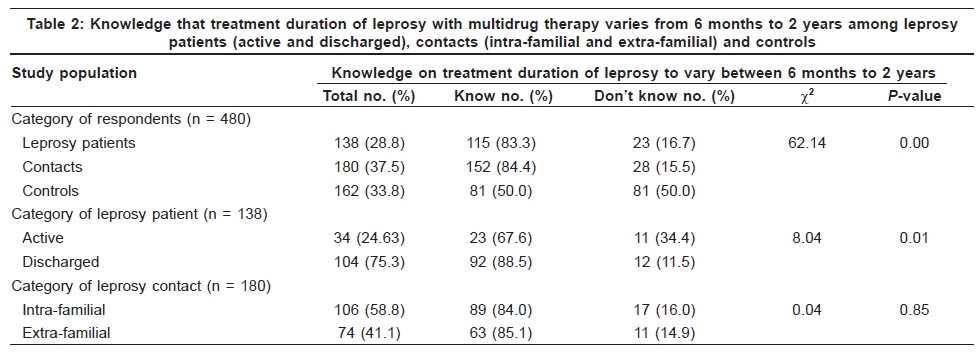
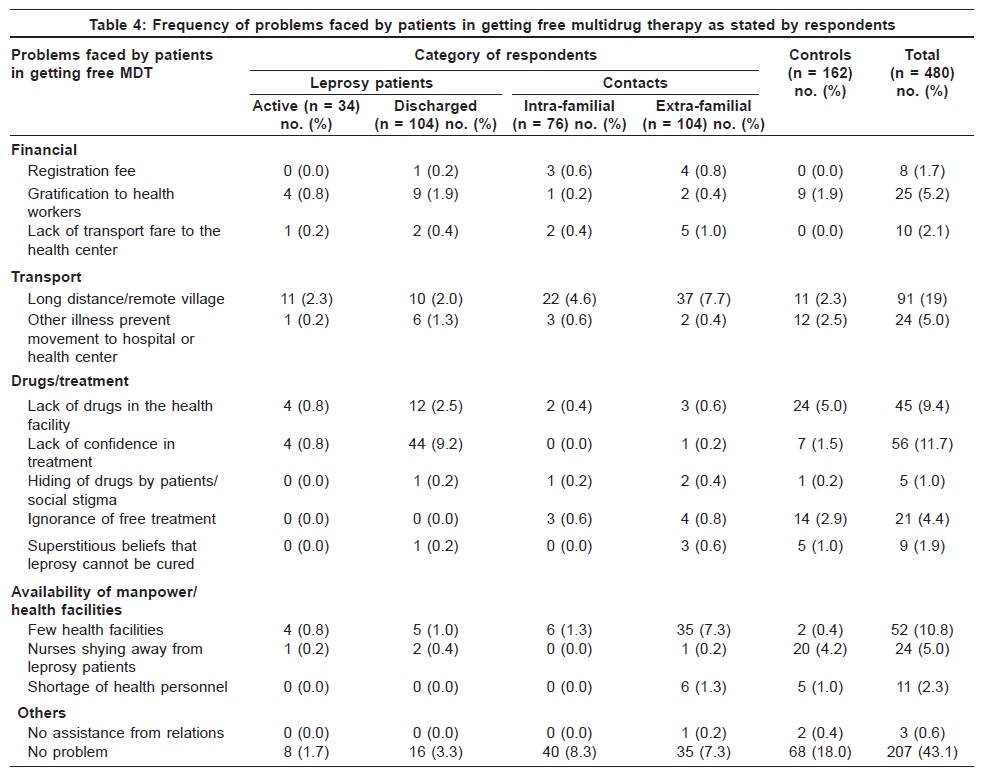
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 469-475 Original Article Operational barriers to the implementation of multidrug therapy and leprosy elimination in Cameroon Dickson S. Nsagha1,2, Elijah A. Bamgboye2, Alain B. O. O. Oyediran2 1Department of Public Health and Hygiene, Medicine Programme, Faculty of Health Sciences, University of Buea, PO Box 63, Buea, Cameroon, Code Number: dv09151 PMID: 19736425 DOI: 10.4103/0378-6323.55389 Abstract Background: The World Health Organization targeted to eliminate leprosy from the world with multidrug therapy (MDT) by 2000. But, leprosy remains a problem in Essimbiland of Menchum Division of Cameroon, with a prevalence of 1.7/10,000 and high rate of case detection in children. Aims: To assess knowledge and practices on the cure of leprosy, treatment duration, drug availability and problems faced by leprosy patients acquiring drugs in order to enhance MDT implementation and leprosy elimination in Menchum and Boyo divisions. Methods: Observational study in which a structured questionnaire was administered to leprosy patients, their contacts and a control group. Results: 480 respondents were interviewed and 405 (84.8%) (95% confidence interval [CI]: 81.6-87.2%) knew that leprosy can be cured. These respondents comprised 166 (92.2%) of 180 contacts, 129 (93.5%) of 138 patients and 110 (67.9%) of 162 controls. Two hundred and fourteen (44.6%) (95% CI: 40.1-48.9%) respondents knew that leprosy treatment is free, comprising of 110 (51.4%) patients, 99 (46.3%) contacts and five (2.3%) controls. A statistically significant difference in the knowledge on free treatment of leprosy was found to exist between leprosy patients, contacts and controls, with leprosy patients having a better knowledge (79.71%) (95% CI: 73-86.42%), followed by contacts (55.0%) (95% CI: 47.73-62.26%) and controls (3.1%) (95% CI: 0.43-5.77%) (P = 0.00). Pertinent problems faced by patients in getting MDT included distant health facilities and poor road network (91[19.0%]), lack of confidence in treatment (56 [11.7%]), MDT shortage (45 [9.4%]), few health facilities (52 [10.8%]), gratification demands (25 [5.2%]), disturbance from other illnesses (24 [5.0]), ignorance (21 [4.4%]) and poor relationship with nurses (24 [5.0%]). Conclusion: Patients still face problems in getting free MDT. Better MDT implementation and leprosy elimination strategies are proposed.Keywords: Barriers, Implementation, Knowledge, Leprosy, Multidrug therapy Introduction In 1980, the drug of choice for leprosy treatment was dapsone but because of widespread resistance, treatment became increasingly ineffective. Also, treatment was life-long, which discouraged the patients. [1] Multidrug therapy (MDT) is a combination of three drugs for multibacillary leprosy and two drugs for paucibacillary cases. [1],[2] MDT enjoys a high degree of patient acceptability, with very low relapse rates following completion of treatment. Compliance is high because of the fixed and relatively short duration of treatment, low frequencies of side-effects, cost-effectiveness and definitive cure in the patient. [3],[4],[5],[6] Despite all these advantages, challenges such as improving MDT coverage in difficult-to-reach areas, completion rates and effective implementation strategies through general health services and primary health care settings exist. [7] The World Health Organization (WHO) targeted to eliminate leprosy as a public health problem from endemic countries by the year 2000, i.e. reducing the prevalence to less than 1 per 10,000. In 2002, leprosy prevalence in Cameroon was 1.35/10,000 and paucibacillary and multibacillary defaulter rates were 22.2% and 37.5% respectively, and detection of new cases was decreasing. [8] But, 574 new cases were detected with 79 child cases giving a prevalence of 0.45/10,000 and a detection rate of 3.71% in 2004. [9] In the enclave Essimbiland, leprosy prevalence was 1.7/10,000 in 2008, [10] with high rate of case detection in children. [11] Deficient knowledge about leprosy and its treatment [12] and ignorance [13],[14],[15] have affected leprosy treatment in Tanzania and other parts of the world. Community participation and behavioral studies can enhance practical understanding of local approaches toward MDT implementation and leprosy elimination. This study was carried out to identify factors that could hinder MDT implementation and leprosy elimination in an endemic region. Methods Study area The study group was drawn from Boyo and Menchum divisions of northwestern Cameroon because they had the highest prevalence of leprosy (3.4/10,000 and 4.5/10,000 respectively). [11],[16],[17] These divisions still have the highest leprosy prevalence (Essimbiland= 1.7/10,000 and Boyo= 2/10,000) in the region. [10] In Boyo division, the study was concentrated in the Mbingo leprosarium and the surrounding villages of Mbingo II, Mejang, Baingo, Dr Jones' quarter and NewHope. In Menchum division, most leprosy patients were in Essimbiland. Because of the inaccessible nature of the terrain, this study was concentrated in Essimbi villages of Benakuma, Benahudu, Benage, Benabenge, Muteege, Atuoh and Vikuru, which had high leprosy prevalence. This study was conducted from June 1998 to October 2002. Inclusion and exclusion criteria for leprosy patients, contacts and controls The leprosy patients were those diagnosed clinically and bacteriologically in health facilities who were either on treatment or discharged cases living in neighbouring villages around the Mbingo leprosarium and in Essimbiland. All intra-familial contacts (wife, children and other relations) and extra-familial contacts (friends, peers, colleagues and villagers) were involved in the study. Controls were those who attended the Bamenda Hospital in Mezam division for reasons other than leprosy. They were selected based on a well-structured, guided questionnaire and those who said they either live or lived with a leper in the same household or quarter were eliminated from the study. Design and setting This was a descriptive observational case-control study that was community based in one low (Mezam division) and two high (Menchum and Boyo divisions) leprosy-prevalent areas. Leprosy patients constituted the cases and the contacts were a high-risk group for developing leprosy. Leprosy patients, their contacts and controls were matched for geographical location, age and sex. Selection technique The list of patients in the study area was established with assistance from health facilities. The patients in the different villages also assisted in the identification of other patients whose names were not in the registers. In the leprosarium, all the available leprosy patients on treatment, those discharged and living within the neighboring villages, including those rehabilitated, were involved. After identifying all the leprosy patients, all their contacts were recruited for the study. A partly open and closed pre-tested structured questionnaire was administered to the respondents. Those who could read or write the English language filled the questionnaire and those who could not were communicated to through an interpreter in Bikom and Essimbi dialects. The questionnaire contained sociodemographic variables on age, sex, marital status, religion, geographical location and profession. Information on the cure of leprosy, duration of chemotherapy, MDT availability and problems patients faced in getting drugs constituted the dependent variables. Ethical approval and clearance The authorization to carry out this work was obtained from the Cameroonian Ministry of Public Health (NºD76/A/MSP/SESP/SG/DRH/SDGP/SFS). Informed consent was sought and gained from all respondents before the questionnaires were administered. Working hypothesis The working hypothesis was that knowledge on MDT was not going to vary among the study and the control groups and the sociodemographic characteristics. Data management and analysis Each time the questionnaires were brought from the field, they were checked for unanswered questions and edited for the use of correct codes and completeness, including range and consistency errors. The data were analyzed using Epi-Info after a double entry by two data clerks. Data summary such as proportions and percentages and testing of the working hypothesis were also carried out using the chi-square and Fisher exact tests for tests of significance of association between categorical variables. Results All 480 respondents comprised 138 (28.8%) leprosy patients and 180 (37.5%) contacts from Boyo and Menchum divisions and 162 (33.8%) controls from Mezam division. Knowledge on the cure and treatment duration of leprosy and demographic characteristics of the respondents Among the 480 respondents who were surveyed, 204 (77.65%) males and 144 (66.45%) females were aware that leprosy can be cured within a specified period with MDT, including 189 (71.9%) married people and 141 (71.6%) singles. Ninety-five (58.3%) farmers, 96 (81.4%) students, 36 (67.9%) with paid employment and 52 (40.9%) self-employed knew that leprosy can be treated within 6 months to 2 years with MDT ( P < 0.05). The 480 respondents comprised of 449 (93.5%) Christians, 10 (2.1%) Muslims and 21 (4.2%) others, but 297 (66.15%) Christians, eight (80%) Muslims and 19 (90.48%) others knew that leprosy treatment is free (χ2 = 60.780, df = 2; P < 0.001). Knowledge on the cure and treatment duration of leprosy Knowledge on the cure of leprosy among leprosy patients, contacts and controls is shown in [Table - 1]. Of the 480 respondents, 405 (84.4%) (95% confidence interval [CI]: 81.6-87.2%) knew that leprosy can be cured ( P = 00). From [Table - 2], 115 (24.0%) leprosy patients, 152 (31.7%) contacts and 81 (16.9%) controls knew that leprosy can be treated within 6 months to 2 years with MDT ( P = 0.00). Two hundred and fourteen (44.6%) (95% CI: 40.1-48.9%) respondents knew that leprosy treatment is free ( P = 0.00). [Table - 3] shows that a statistically significant difference in knowledge on free treatment of leprosy was found to exist between leprosy patients, contacts and controls, with leprosy patients having better knowledge (79.71%) (95% CI: 73-86.42%), followed by contacts (55.0%) (95% CI: 47.73-62.26%) and controls (3.1%) (95% CI: 0.43-5.77%) ( P =0.00). From [Table - 4], the most pertinent problems cited by the respondents in getting drugs were long distance to the health facility (91 [19.0%]), lack of confidence in treatment (56 [11.7%]), few health facilities (52 [10.8%]), lack of drugs (45[9.4%]), demand for gratification by health workers (25 [5.2%]), nurses shying away from leprosy patients (24 [5.0%]) and ignorance of free treatment (21[4.4%]) (by ignorance, we mean the respondents were not aware that leprosy treatment is free). Most of these problems were cited more frequently by leprosy patients (119 [86.2%]) and their contacts (148 [82.2%]) than by controls (101 [62.3%]). The problems were grouped into four categories: financial, transport, drugs/treatment and availability of manpower/health facilities for easy analysis and discussion (others included problems such as abandonment of a leprosy patient by family members in the leprosarium that could not fit into the above four categories). An overview of all the problems according to categories reveal that problems linked to drugs/treatment were the most frequent (136 [28.4%]), followed by transport (115 [24.0%]), availability of manpower/health facilities (87 [18.1%]) and finance (43 [9.0%]). The figures in the table indicate the number of times these problems were mentioned by respondents. Discussion This study has shown that investigations on knowledge and behavior of people on the cure, treatment duration and MDT availability can enhance practical understanding of local approaches toward improving health care delivery and in developing broader-based implementation strategies for leprosy control. Leprosy was integrated into primary health care in Cameroon in 1991 but it became operational in Essimbiland after 1998 and it is intensified by flyer sensitisation, case detection and MDT treatment with assistance from the Mbingo leprosarium. For the elimination of leprosy as a public health problem from Essimbiland, the barriers identified in this study coupled with a high level of illiteracy (32.1% for adults), poverty (human poverty index of 31.8), cultural taboos (isolation of patients in the bush), low socioeconomic potentials (95% of the population are peasant farmers) and poor housing (one room with many occupants) need to be addressed because these determinants were used to eliminate leprosy from Japan, Europe and many other developed countries long before the advent of chemotherapy. Because leprosy patients live in the Mbingo leprosarium and the neighboring villages of Boyo, Menchum and Mezam divisions, this study thus contributes to identifying obstacles and proposing innovative ways that can lead to the elimination of leprosy in these communities. Knowledge of MDT treatment of leprosy within 6 months to 2 years Most participants knew that leprosy can be cured, but knowledge on MDT treatment duration was generally low. The leprosy patients know MDT and tend to master its duration of administration than contacts and controls. The discharged patients who have completed treatment may tend to know more about MDT duration than active patients. Knowledge of free treatment of leprosy among the subjects Lack of awareness by most respondents of free leprosy treatment can be a serious hindrance to elimination, especially in the enclave Essimbi. In remote areas, leprosy patients could spend some time sourcing for money before coming to the hospital for treatment because they were ignorant of free MDT, hence constituting infection pools. Sensitization campaigns on free MDT involving health facilities, local and international non-governmental organizations are necessary. In Cameroon, men have the responsibility of providing funds for the treatment of sick members of their nuclear and extended families. Men are therefore more likely to find out from the sick ones or health officials on the effectiveness of treatment and on the type of disease the person is suffering from. Men are principal motivators and providers in the welfare of the family and hence their better knowledge on the cure of leprosy and treatment duration. Problems faced by leprosy patients in getting MDT and implications for elimination Financial problems The most pertinent financial problem was the demand for gratification by some health workers followed by registration fee and lack of transport to the health center. The demand for gratification is a problem that can be solved by involving village chiefs, churches and opinion leaders in the distribution of MDT. Registration fee at the leprosarium and lack of transport money to the health center are factors that can affect elimination of leprosy and contribute to default and MDT implementation. Also, the threat to patients who have managed to get to the leprosarium to go back home and bring the registration fee of 10,000 francs CFA (about USA 20 dollars) may lead to default. In the leprosarium, the registration fee could be waived for the patients because some of the poor leprosy patients might not be able to afford it. In remote areas like Essimbiland, patients without a means of transportation to health facilities might constitute infection pools, which can slow down leprosy elimination. Transport Long distance or remote village was cited by 19.0% of the respondents, especially in the enclave Essimbiland where a lot of trekking is required. Improving the socioeconomic development of a community is a major driving force in the elimination of leprosy, as evidenced by the elimination of leprosy from developed countries long before the advent of chemotherapy.[19] Road construction to this enclave region could bring development, ease MDT implementation and accelerate leprosy elimination, but this seems far fetched because the road construction may involve many other factors apart from leprosy. Drugs/treatment Problems pertaining to drugs/treatment were the most pertinent of all the problems cited, the most common of which was lack of confidence in treatment maybe because of the 6 months to 2 years treatment duration that some consider long (personal communication by lead author with leprosy patients) compared with diseases like malaria that can be treated within days. This falls in line with one of the recommendations of the WHO Expert Committee on leprosy to reduce the treatment duration of the disease. [20] Some leprosy patients treated years ago still develop deformities, which has forced many other patients to doubt the effectiveness of the treatment and by implication may not take MDT, which can hinder the elimination struggle. Identifying causes is often a first step toward treatment of diseases. In the study area, when somebody is affected by leprosy, the family searches for the cause of the disease, in the majority of the cases not linked to orthodox medicine. When the family concludes that the disease can be cured, treatment is sought with more seriousness. But, when the family concludes that the condition cannot be changed, may be the patient's "hand" is involved (superstitious beliefs), the patient is abandoned in the leprosarium. As Whyte and Ingstad [21] put it, "it is at this point that people in East Africa begin to speak of the 'work of God,' unalterable by the efforts of humans." With such beliefs, patients may not take MDT because they "know" they will not be cured. Lack of MDT in hospitals may be due to other logistics or administrative bottlenecks because MDT is provided free of cost by the WHO. Other pertinent problems stated by the subjects included ignorance that leprosy treatment is free, superstitious beliefs that leprosy cannot be cured and the hiding of drugs by patients. Poor knowledge about leprosy treatment [12] and ignorance [13],[14],[15] have been reported as reasons affecting leprosy treatment in Tanzania and other parts of the world. These findings indicate that health education is much needed in leprosy treatment in order to facilitate MDT implementation and elimination. Availability of manpower/health facilities Leprosy has been integrated into primary health care in Cameroon, [16],[17],[19] but there are many remote areas without health centers. Shortage of health personnel was commonly observed as well as stated by the respondents. The Mbingo leprosarium managed by two nurses and one doctor and the Benakuma health center managed by one itinerant is certainly insufficient to take care of all patients. More health workers need to be trained to go to the community and look for new patients, coordinate and supervise MDT implementation to win the battle of elimination. Conclusions Leprosy patients still face problems in getting free MDT. Information on the cure of leprosy, duration of chemotherapy and that leprosy treatment is free should be disseminated to the general public through the radio, posters, television and print media. Working in collaboration with local communities, waiving of registration fees before treatment and deployment of more health personnel to the enclave Essimbiland would be good. Consultants from countries with successful MDT implementation programmes could be sought for effective strategies to enhance elimination. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09151t3.jpg] [dv09151t4.jpg] [dv09151t1.jpg] [dv09151t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}