 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
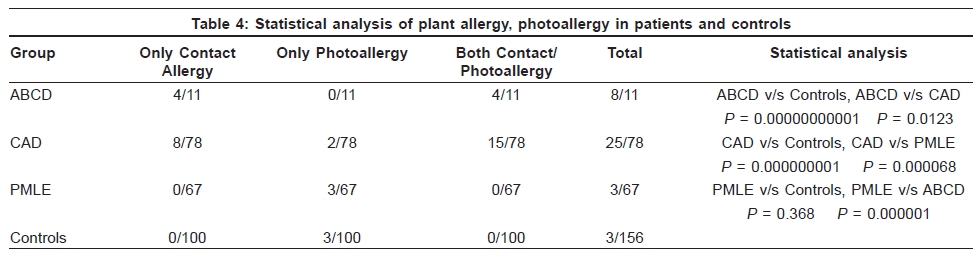
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 483-487 Original Article Occurrence of plant sensitivity among patients of photodermatoses: A control-matched study of 156 cases from New Delhi Hemanta Kumar Kar, Sonali Langar, Tarlok Chand Arora, Pankaj Sharma, Alok Raina, Meenakshi Bhardwaj1 Departments of Dermatology and 1Histopathology, Dr. Ram Manohar Lohia Hospital, New Delhi, India Correspondence Address: Dr. H K Kar, Department of Dermatology, Dr. Ram Manohar Lohia Hospital, New Delhi-110001, India Code Number: dv09153 PMID: 19736427 DOI: 10.4103/0378-6323.55391 Abstract Background: Photodermatitis is an abnormal response to ultraviolet radiation (UVR). The photoallergic contact dermatitis caused by plant allergens is a serious cause of morbidity in India. Airborne contact dermatitis is the classical presentation of plant-induced dermatosis, which may become difficult to differentiate from chronic actinic dermatitis in chronic cases. The rapid growth of parthenium weed in India and its ill effects on the population make it important to detect all cases of parthenium sensitivity, which in some cases might simulate photodermatitis.Aims: This study aims to detect the occurrence of plant sensitivity and photosensitivity in idiopathic-acquired photodermatoses, airborne contact dermatitis and general population taken as controls. Methods: One hundred and fifty six consecutive patients suffering from polymorphic light eruption (PMLE), chronic actinic dermatitis (CAD) and airborne contact dermatitis (ABCD) were enrolled in the study over a period of three years (June 2004 to May 2007). An equal number of age and sex matched healthy subjects were enrolled in the study as controls. All the patients were subjected to detailed history taking, clinical examination and histopathological examination for diagnosis. Patch and photopatch testing were perfomed in all the patients and healthy controls for detection of allergic and photoallergic reactions to parthenium, xanthium and chrysanthemum plant antigens and control antigens. Results: Out of 156 patients enrolled in the study, 78 (50%) had CAD, 67 (42.9%) had PMLE and 11 (7.05%) had ABCD. The occurrence of parthenium/xanthium allergy and photoallergy, either to parthenium or both was most commonly found in ABCD (72.7%), followed by CAD (32%). In PMLE 4.5% cases showed photoallergy. Only 1.9% in the control group showed sensitivity to parthenium and xanthium. Conclusion: This study indicates that parthenium (and possibly xanthium) may act as important environmental factors in the initiation and perpetuation of not only ABCD but of CAD as well. Photoexacerbation to UVA at positive parthenium/xanthium sensitivity sites in ABCD and CAD indicates that ABCD with photosensitivity to compositae can lead to CAD. Keywords: Photodermatosis, Plant sensitivity, Airborne contact dermatitis Introduction Photodermatitis is an abnormal response to ultraviolet radiation (UVR). Clinically it can be divided into four groups: Idiopathic, photoallergic/phototoxic, metabolic/genetic and dermatoses exacerbated by UV light. [1] The photoallergic contact dermatitis caused by plant allergens is a serious cause of morbidity in India. The initial classical presentation of plant-induced dermatosis is the airborne contact dermatitis (ABCD), which may become chronic and clinically difficult to differentiate from chronic actinic dermatitis (CAD). Parthenium dermatitis simulating photodermatitis has been reported by various authors. [2],[3] The rapid growth of parthenium weed in India and its ill effects on the population makes it important to detect all cases of parthenium dermatitis, which in some cases might simulate photodermatitis and thus manage them accordingly. The aim of the present study was to evaluate the occurrence of plant sensitivity and photosensitivity in patients of idiopathic photodermatoses, airborne contact dermatitis and general population taken as control. Methods One hundred and fifty six consecutive patients suffering from polymorphic light eruption (PMLE), chronic actinic dermatitis (CAD) and airborne contact dermatitis (ABCD) were enrolled in the study over a period of three years (June 2004 to May 2007) from the outpatient dermatology department of Dr. Ram Manohar Lohia Hospital, New Delhi. An equal number of age and sex matched healthy subjects (with no history of photodermatoses) were enrolled in the study as controls. All the patients were subjected to detailed history taking, clinical examination and histopathological examination for diagnosis. The patients' details recorded included age, sex, type of occupation, average number of hours of sunlight exposure in a day, response to sun exposure, age of onset of disease, duration of disease, history of seasonal variation, history of drug intake and family history. Findings of clinical examination were recorded separately for both exposed and covered sites. Histopathological examination of the cutaneous lesion was done in all the cases. Patch and photopatch testing were performed in all the patients and healthy controls for detection of allergic and photoallergic reactions to parthenium, xanthium and chrysanthemum plant antigens and control antigens using readymade plant antigen strips with antigen-impregnated-discs (supplied by Systopic labs, New Delhi) as per the guidelines approved by the Contact and Occupational Dermatosis Forum of India (CODFI). The strips were applied in duplicate, both sets were read at 48 h. One set was covered with opaque plaster and the other set was irradiated with UVA radiation (10 J/cm 2 ) using hand and foot treatment unit. The photopatch site was covered again and both sets were read at 96 h. The patch and photopatch test reactions were read according to the recommendations made by the International Contact Dermatitis Group (ICDRG). Interpretation of photopatch test at 96 h is shown in [Table - 1]. Data obtained was compiled, tabulated and statistically summarized. Occurrence of plant sensitivity in idiopathic photodermatoses was compared with that of ABCD and controls. The comparison was made using Chi-square test. Results Out of 156 patients enrolled in the study, 78 (50%) had CAD, 67 (42.9%) had PMLE and 11 (7.05%) had ABCD. The age of patients (76 males, 80 females) and controls (78 males, 78 females) were between 18 and 70 years of age. The median age of patients having ABCD, CAD, PMLE and controls were 50.7, 48.5, 32 and 32.5 years, respectively. In ABCD group, a marginally higher number of patients 6/11 (54.5%) were engaged in outdoor work while those in CAD 26/78 (33.3%) and PMLE 13/67 (19.4%) had occupations involving outdoor activities. In the control group, 121/156 (71.2%) were engaged in indoor occupation. The average daily sun exposure was 4.75 h in ABCD group, 3.5 h in CAD and 3.8 h in PMLE. In control group, the average daily sun exposure was 3.4 h. Sun exposure lead to exacerbation of disease in 81.4% of patients, out of whom 10/11 (90.9%) had ABCD, 66/78 (84.6%) had CAD and 51/67 (76.1%) had PMLE. The mean age of onset of disease was 44.75 years in ABCD, 46.5 years in CAD and 30.04 years in PMLE. The average duration of illness was 6 years in ABCD, followed by 2 years in CAD and 1.96 years in PMLE. Exacerbation of disease was seen in summer in 78/156 (50%) patients, in both summer and rainy season in 11/156 (7%), only rainy season in 3/156 (2.1%) and winter exacerbation in 5/156 (3.5%) cases. A substantial number of patients, 55/156 (35.2%), did not notice any change in disease pattern with any season. Five percent of the patients gave history of drug intake of nonsteroidal anti-inflammatory drugs and furazolidine while none of the control group subjects gave such history. Clinically, patients of ABCD presented with erythematous papules and plaques on exposed areas, such as the face, upper eyelid, sides of neck, V of chest, flexures of forearm and cubital fossa. Patients with CAD had eczematous lichenified plaques on the exposed sites and PMLE patients presented with erythematous papules and plaques (few showing vesicles) on the sun-exposed regions of the body. The biopsies taken from all the patients showed histopathological changes of chronic nonspecific dermatitis. The overall occurrence of plant sensitivity in the patient group was seen in 36 (23.1%) cases with 28 (17.9%) showing sensitivity to parthenium alone, 5 (3.2%) showing sensitivity to both parthenium and xanthium and 3 (1.9%) showing sensitivity to all three plant antigens. Thus parthenium sensitivity was universally present in the reactive patients. Isolated xanthium and chrysanthemum sensitivity was not seen in any patient [Table - 2]. The occurrence of plant sensitivity in the control group was seen in only 3 (1.9%) cases who showed photo contact allergy (two to parthenium alone and one to parthenium and xanthium). In the ABCD group, 4/11 (36.3%) cases each, showed contact allergy and both contact allergy and photoallergy to parthenium. Thus among ABCD patients, 8/11 (72.7%) cases showed plant sensitivity. In CAD group, 25/78 (32%) cases showed parthenium sensitivity out of which 8/78 (10.2%) cases showed contact allergy, 2/78 (2.6%) cases showed photoallergy and 15/78 (19.2%) cases showed both contact allergy and photoallergy to parthenium. Only 3/67 (4.5%) cases of PMLE showed photoallergic reaction to parthenium [Table - 3]. The male and female distribution did not show any statistically significant difference in our study. The statistical analysis of parthenium allergy, photoallergy, and combined allergy and photoallergy among idiopathic photodermatoses group (CAD and PMLE), ABCD group and control group is shown in [Table - 4]. Discussion Photodermatitis is an abnormal response to ultraviolet radiation (UVR). Clinically it can be divided into:
Most cases of airborne dermatitis in India are considered to be due to parthenium. [7] Sharma and Kaur recorded 78% of ABCD patients having parthenium sensitivity.[8] In our study 8/11 (72.7%) ABCD cases showed parthenium sensitivity out of which 4/11 (36.4%) had photoallergy to parthenium. Sharma et al . in their study found 3/9 photopatch tested patients with photoallergic reaction to parthenium and another three patients showed photoaggravation.[2] The prevalence of plant sensitivity in CAD was reported to be 47/55(85.5%) in a study from Canada.[9] However, Somani reported 3/9 (33.3%) CAD patients with parthenium sensitivity with 2/9 (22.2%) patients showing photoallergy to parthenium.[10] In the present study, 25/78 (32%) CAD patients showed parthenium sensitivity of whom 17/78 (21.7%) showed photoallergic reaction to the weed. The mean age of onset of CAD in the same study was 47.5 years and in our study it was 46.5 years. No specific studies indicating the occurrence of plant sensitivity in PMLE could be found in literature. In the present study, it was found in 3/67 (4.5%) patients. However, this was not found to be statistically significant as compared with that of controls ( p < 0.368). In Europe, the prevalence of plant sensitivity varies from 0.7 to 1.4% in the general population. [11] Occurrence of plant sensitivity in the general population is not known in India. In our study, it was seen in 3/156 (1.9%) of controls. ABCD and CAD have traditionally been considered to be primarily affecting males and PMLE affecting females. The male affliction in our study was 9/11(82%) in ABCD, 44/78 (56.4%) in CAD and 21/67(31.3%) in PMLE. Studies from West have reported a male preponderance as high as 20 : 1 in case of ABCD. [12],[13] However, studies from India have shown a male : female ratio of 1 : 1.[14] An almost equal ratio was also seen in the present study. The present study indicates that the occurrence of plant sensitivity is highest in ABCD, followed by CAD. Thus parthenium (and possibly xanthium) may act as important environmental factors in the initiation and perpetuation of not only ABCD but of CAD as well. In PMLE, compositae plant antigens do not seem to play any role as environmental agents. Photo exacerbation to UVA at positive parthenium/xanthium sensitivity sites in ABCD and CAD indicates that ABCD with photosensitivity to compositae can lead to CAD. Acknowledgement This Research project was supported by a financial grant from Department of Biotechnology (DBT), Ministry of Science and Technology, Government of India. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09153t4.jpg] [dv09153t2.jpg] [dv09153t1.jpg] [dv09153t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}