 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
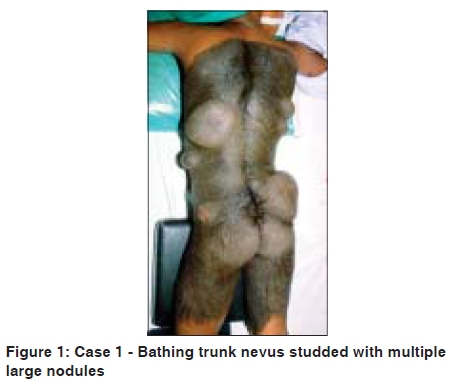
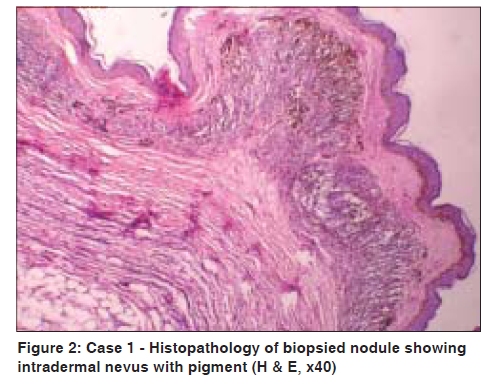
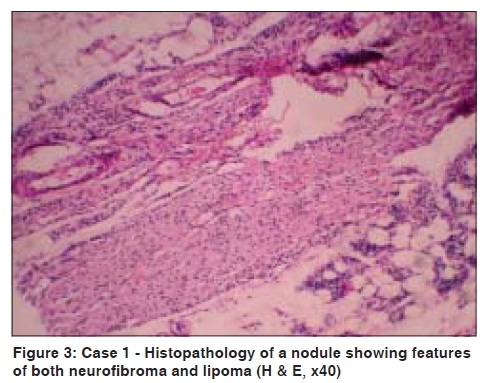
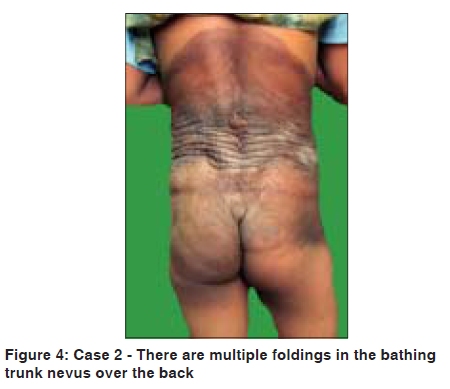
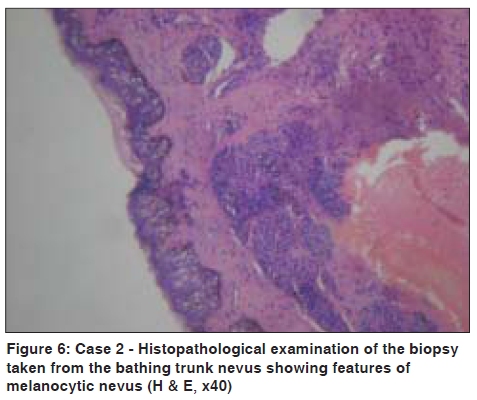
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 495-498 Case Report Giant congenital melanocytic nevus (bathing trunk nevus) associated with lipoma and neurofibroma: Report of two cases P. V. Bhagwat, R. S. Tophakhane, B. M. Shashikumar1, Tonita M. Noronha, Varna Naidu Department of Skin and STD, Karnataka Institute of Medical Sciences, Hubli, Karnataka, 1 Mandya Institute of Medical Sciences, Mandya, Karnataka, India Code Number: dv09156 PMID: 19736430 DOI: 10.4103/0378-6323.55394 Abstract Giant congenital melanocytic nevi are rare and occur in about one out of every 2,00,000 to 5,00,000 births. There is a significant association between bathing trunk nevus and neurofibromatosis and lipomatosis. Apart from this, association of bathing trunk nevus with abnormalities like spina bifida occulta, meningocele, club foot and hypertrophy or atrophy of deeper structures of a limb, have been described. We are herewith reporting two cases of bathing trunk nevi. In our first case, an eight-year-old girl presented with a bathing trunk nevus studded with multiple, large nodules. Histopathological examination of the biopsy taken from one nodule revealed features of both neurofibroma and lipoma. To the best of our knowledge, features of both these hamartomas in one nodule of a single patient are probably not reported in the literature. In our second case, a 12-year-old girl presented with bathing trunk nevus and she had spina bifida occulta. She also had lipoma in the lesion of bathing trunk nevus. Both of our patients had satellite melanocytic nevi over the face, forearm, upper back and legs. Our second patient, in addition, had small melanocytic nevi over the medial canthus and sclerocorneal junction of the right eye. By the time this girl presented to us, the melanocytic nevus started fading in color and it had become brownish. We are reporting these cases for their peculiarities and for their rare features.Keywords: Bathing trunk nevus, Lipoma, Neurofibroma Introduction Congenital melanocytic nevus is a benign neoplasm composed of nevomelanocytes, which occurs in about 1 to 2% of newborns. Giant congenital melanocytic nevus is a variant of congenital melanocytic nevus, characterized by its extensive size and is defined as melanocytic nevus measuring more than 20 cm in its greatest dimension . These are uncommon birthmarks, occurring in approximately one in 2,00, 000 to 5,00, 000 births, with a female predominance. [1] These giant nevi often have a garment-like distribution. They are usually deeply pigmented, covered with moderate growth of hair and often there are many scattered satellite lesions associated with them. The hairy component, which occurs in 95% of lesions, tends to become more prominent in late childhood but at this stage, the nevus becomes paler. [2] Malignant neuroectodermal tumors and malignant melanoma might develop in the lesion of a giant congenital melanocytic nevus . Bathing trunk nevus may also be associated with several conditions like neurocutaneous melanosis, diffuse lipomatosis, von-Recklinghausen's disease, vitiligo, structural brain malformations, hypertrophy of skull bones and skeletal asymmetry. [3] We are herewith reporting two cases of garment nevi with multiple, peculiar findings. Case Reports Case 1 An eight-year-old girl, resident of Kalaghatagi near Hubli of Dharwad district in Karnataka, presented to us with large, blackish skin lesions covered with thick, black, long hairs over the entire lower three fourths of the trunk and up to the knee level, encircling the entire area circumferentially, since birth. Initially, the lesion was flat and gradually it became thicker. Gradually, thick, black, long hairs developed in the lesion. At the age of five years, she developed multiple, asymptomatic nodules in the lesion, which gradually increased in size over the last three years to attain the present size. There was no other significant history. Nobody in her family had similar complaints. Her general physical examination and systemic examination including musculoskeletal examination was within normal limits. Cutaneous examination revealed a large, blackish, thick plaque, covering the entire lower three-fourths of the trunk, extending up to the knee level, encircling the trunk circumferentially. The plaque was covered with thick, black hairs, measuring 5-8 cm in length, more marked over the thighs. There were multiple nodules, the smallest being about 10 cm in diameter, present over the left flank, and the largest being about 20 cm in diameter, present over the left infrascapular area and right gluteal region [Figure - 1]. The nodules were non-tender with a smooth surface. These nodules were firm in consistency and mobile only along the horizontal plane, whereas they had restricted movement along the vertical plane. These nodules were distributed over the back and the gluteal region. There were no such nodules over the chest, abdomen and anterior aspect of thighs. There were multiple, blackish papules and plaques measuring from 3 mm to 4 cm in diameter, distributed over the forearms, face, upper chest and legs. Mucosal surfaces, hair and nails, palms and soles were normal. Ophthalmological examination was normal. On investigation, complete hemogram, biochemical parameters, urine routine examination, X-ray of the vertebral spines and computerized (CT) scan of the brain were all normal. Biopsy was taken from one of the nodules which on histopathological examination demonstrated intradermal nevus with pigment. [Figure - 2]. The nevus cells were arranged in groups and sheets in the upper dermis. The nevus cells were also seen infiltrating the deeper dermis, thickened subcutaneous fat and around blood vessels. Also seen were areas showing features of both neurofibroma and lipoma [Figure - 3]. The patient was referred to a pediatric surgeon for excision of the nodules. Case 2 A twelve-year-old girl, resident of a village in Dharwad district of Karnataka, presented with asymptomatic, large, brownish skin lesion covering the entire lower part of trunk, genital region and upper thighs. The lesion was present since birth. Initially the lesion was blackish in color and was flat. Gradually, the lesion thickened and got elevated above the skin surface and developed into folds, especially over the back. The color of the lesion gradually faded to become brownish, and thick terminal hairs started growing on the surface of the lesion. She observed that the lesion increased in size proportional to her growth. She noticed for the past two years, that a few asymptomatic nodules have started to appear over the back in the nevus. These nodules were initially small, the size of a peanut, but gradually increased in size. The girl was born of second degree consanguineous marriage and there was no family history of similar disorder. She had not yet attained menarche. Her general physical examination did not reveal any abnormality except that she had hypertrichosis in the lower back and there was a dimple in the hypertrichotic area over the lower back. Her systemic examination was unremarkable. Ophthalmological examination was normal. Cutaneous examination revealed a large, hyperpigmented plaque, covering the entire lower part of the abdomen, encircling the back and extending up to the upper part of the thigh and genitalia. The lesion over the lower back had multiple folds [Figure - 4]. There were multiple, non-tender smooth nodules, measuring 4-8 mm, soft, mobile, slipping under the palpating fingers, distributed over the back and the right side of the chest on the lateral aspect. There was hypertrichosis over the hyperpigmented plaque, more marked over the left thigh. The hairs were thick and terminal. There were multiple, blackish papules measuring 3-5 mm, and plaques measuring 2-3 cm, distributed over the cheeks, forearms, upper back and legs. There were two blackish papules, one over the medial canthus and one over the sclero-corneal junction of the right eye. Mucosae, hair, nail and palms and soles were normal. On investigation, complete hemogram, biochemical parameters and urine routine examination were normal. X-ray of the lumbosacral spine revealed spina bifida occulta [Figure - 5]. CT scan of the brain was normal. The pigmented nevus was biopsied and subjected to histopathological examination which revealed features of melanocytic nevus [Figure - 6]. Biopsy was done from the nodule over the right side of the lateral aspect of the chest which revealed features of lipoma. Discussion There are several reports of the association of garment nevus with lipoma, neurofibroma and spina bifida occulta. [2],[4] In a report, a 12-year-old girl presented with garment nevus which involved the entire body including the oral mucosa. She had multiple neurofibromatosis and spina bifida occulta. [4] In another case report, a 21-year-old white male patient with bathing trunk nevus studded with neurofibroma-like papules has been described. [5] In yet another case report, a case of giant congenital nevomelanocytic nevus with satellite lesions, vitiligo and lipoma has been described. The authors have explained the constellation of these findings on the basis of a defect in the neural crest, which is considered to be a common origin of melanoblasts, Schwann cells, sensory ganglia, bone, fat, muscle and blood vessels.[6] In both our cases, mucosae were spared. Our first case was a very special one, in that the patient had bathing trunk nevus studded with big nodules and on histopathological examination of one of the biopsied nodules revealed features of both neurofibroma and lipoma, which, to the best of our knowledge, has not been reported in the literature. She did not have spina bifida occulta. Our second patient had bathing trunk nevus studded with multiple lipomas and she also had spina bifida occulta. She did not have neurofibromas. In a study done on agouti mouse, the authors investigated a possible role of the central nervous melanocortin system in the control of adiposity through effects on nutrient partitioning and cellular lipid metabolism independent of nutrient intake. Central nervous melanocortin system, the most potent brain circuit known to control food intake, also directly regulates peripheral lipid metabolism. The melanocortin neurons and melanocortin receptors in the central nervous system directly and potently affect cellular glucose utilization, lipid uptake and triglyceride synthesis in the periphery. This most likely occurs through effects on the autonomic outflow, thereby efficiently shifting substrate metabolism to modulate energy storage and adiposity. The authors of this study conclude that largely independent of changes in food intake, the central nervous melanocortin system directly and rapidly controls triglyceride synthesis, lipid deposition and lipid mobilization in white adipose tissue. The sympathetic nervous system connects white fat cells directly with homeostatic control areas in the central nervous system, including melanocortin-positive neurons in the hypothalamus as well as in other non-hypothalamic forebrain areas, midbrain and brainstem areas. The central nervous melanocortin system modulates sympathetic nerve activity in white adipose tissue and that sympathetic nervous system signaling via functional β-adrenergic receptors is required for the central nervous melanocortin system-induced changes in adipocyte metabolism.[7] These mechanisms may explain the occurrence of lipoma in giant congenital melanocytic nevus. There are pluripotent stem cells in the dermis and subcutis, which, on appropriate stimulus, differentiate into a specific tissue. This would probably explain the occurrence of both lipoma and neurofibroma in a single nodule. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09156f5.jpg] [dv09156f1.jpg] [dv09156f6.jpg] [dv09156f2.jpg] [dv09156f4.jpg] [dv09156f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}