 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
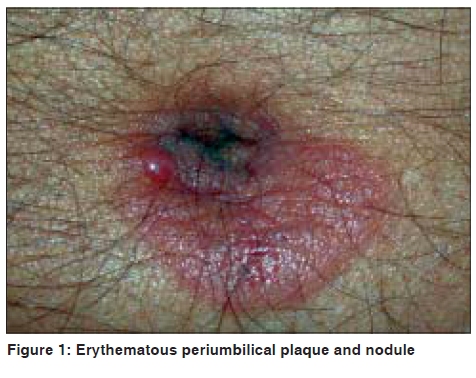
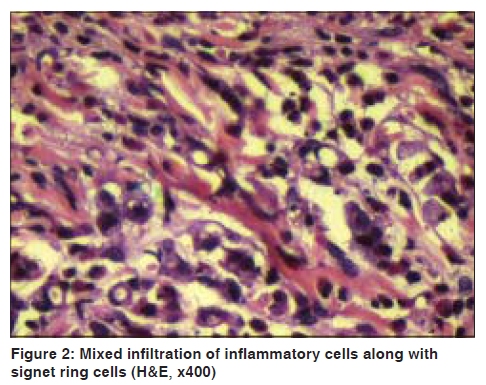
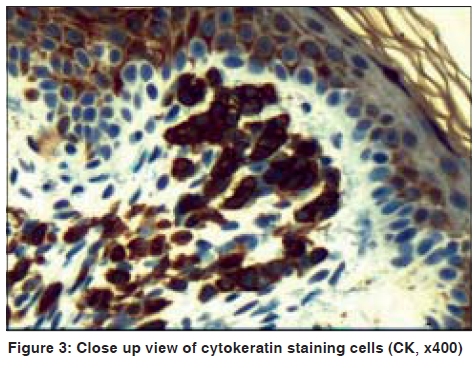
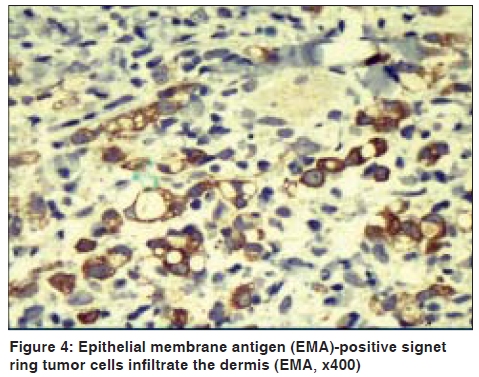
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 503-505 Case Report Sister Mary Joseph's nodule: A case of umbilical cutaneous metastasis with signet ring cell histology Valid Bagher Zadeh, Randhir Kadyan, Adel Al-Abdulrazzaq, Sultan Al-Otaibi, Amr Sarhan, Nabeel Najem Department of Dermatology, Adan Hospital, Kuwait Code Number: dv09158 PMID: 19736432 DOI: 10.4103/0378-6323.55396 Abstract The metastasis of a visceral malignancy to the umbilicus is known as "Sister Mary Joseph's nodule". It is a rare clinical sign indicating advanced, metastasizing intraabdominal cancer. We report a 50-year-old man who developed metastatic skin cancer in the form of semicircular indurated plaque on top of which was a firm mobile rounded nodule at the umbilical area. Histopathological examination demonstrated diastase-resistant periodic acid-Schiff and mucicarmine positive signet ring cells, suggesting gastric carcinoma. Immunohistochemical staining showed that these cells were positive for cytokeratins and epithelial membrane antigen, suggesting epithelial origin.Keywords: Cutaneous metastasis, Sister Mary Joseph's nodule, Signet ring cell Introduction Umbilical metastasis (Sister Mary Joseph's nodule), named by Hamilton Bailey after Sister Mary Joseph, is a rare physical sign encountered in 1−3% of the patients with intraabdominal and/or pelvic malignancy, with gastric carcinoma being the most common origin in men and ovarian carcinoma in women. [1],[2],[3],[4],[5] Signet ring cells, when seen in a metastatic skin deposit, may indicate that the primary tumor is from the stomach or colon. We report a patient whose metastatic skin cancer was characterized by many mature signet ring cells invading the dermis. Case Report A 50-year-old man presented with a single asymptomatic skin lesion around the umbilicus of one-month duration. Examination revealed erythematous semicircular indurated plaque attached to the lower part of the umbilicus which was neither painful nor tender. On top of the plaque, there was a single erythematous firm mobile rounded nodule about half centimeter in diameter [Figure - 1]. Abdominal palpation did not reveal liver, spleen or lymph node enlargement. His full blood count and blood biochemistry studies were normal. No abnormalities were seen on urine and stool examination. Chest X-ray did not show any significant findings. Alpha-fetoprotein, carcinoembryonic antigen, prostate-specific antigen, CA 125 and CA 19-9 were all within normal limits. Histopathological examination revealed variable fibrosis and diffuse chronic inflammatory infiltrate in the dermis. Lower and deep dermis showed few clusters of pleomorphic small cells with hyperchromatic nuclei, many of which showed signet ring appearance [Figure - 2]. These signet ring cells were not digested with diastase and were positive both for periodic acid-Schiff (PAS) reagent and mucicarmine. Immunohistochemical studies showed that these cells were positive for cytokeratins (CK) and epithelial membrane antigen (EMA) [Figure - 3] and [Figure - 4]. They were negative for vimentin, S-100 protein, gross cystic disease fluid protein-15 (GCDFP-15; BRST-2), and leukocyte common antigen (LCA; CD45) staining. These features define the epithelial origin of the neoplastic cells. The patient was referred to Kuwait Cancer Control Center (KCCC), where abdominal computerized tomographic scan and ultrasound, fluoroscopy and endoscopic examination revealed a gastric carcinoma. Discussion Sister Mary Joseph (1856−1939), who was superintendent nurse at St. Mary's Hospital in Rochester, MN, US (at present, the Mayo Clinic), observed that patients with intraabdominal and/or pelvic malignancy occasionally have an umbilical nodule indicating umbilical metastasis. Consequently, in 1949, the English surgeon Hamilton Bailey in his famous textbook "Demonstrations of physical signs in clinical surgery" coined the term "Sister Mary Joseph's nodule" for umbilical metastasis. [1] Although skin metastasis is rare and ranges between 5% and 9%, it is estimated that 1% to 3% of abdomino-pelvic tumors metastasize to the umbilicus. Metastatic tumors of the umbilical region, constitute 83% of all malignant umbilical tumors and are much more common than primary malignant tumors of this area. [2],[3],[4],[5] The histologic nature of metastatic umbilical tumors usually suggests adenocarcinoma; however, there have also been reports of umbilical metastases from sarcoma, mesothelioma, and melanoma. [6],[7] In men, gastrointestinal tract is the most common location of the primary neoplasm that metastasizes to the umbilicus, whereas in women gynecological neoplasms particularly ovarian cancer is the most common primary site. [2],[3],[4] Sister Mary Joseph's nodule may be painful and ulcerated, sometimes with pus, blood or serous discharge. It is usually a firm nodule measuring 0.5−2 cm, although some nodules may reach up to 10 cm. [4] Since Sister Mary Joseph's nodule is usually a reflection of an underlying widespread malignancy, patients with this sign have a poor prognosis with life expectancy of less than one year. [8] Signet ring cells contain a large amount of mucin because of the production of mucin without an outlet. The nucleus, pressed to one side of the cell, appears crescent-shaped and the cell looks like a signet ring. These cells are seen in mucous-producing carcinomas such as those from the stomach, colon, and bladder. [9] In gastric carcinoma, which is classified histologically into adenocarcinoma, mucoid carcinoma and diffuse carcinoma, the frequency of signet ring cell carcinoma ranges between 2−3.4%. [10],[11] However, 16−20% of skin metastases from stomach cancers are from signet ring carcinomas, suggesting that this histological type has either a greater tendency towards distant metastasis or greater likelihood of becoming differentiated in the skin than in the stomach. [12] Acknowledgments We are thankful to Dr. Munish Joneja (Department of Histopathology at Radiology, Nuclear Medicine and Laboratory Center, YIACO Medical Co., KSCC) for the histopathological and immunohistochemical studies. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09158f4.jpg] [dv09158f2.jpg] [dv09158f1.jpg] [dv09158f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}