 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
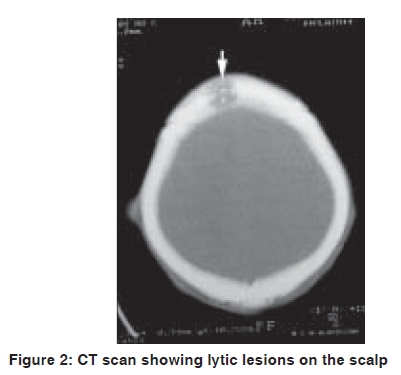
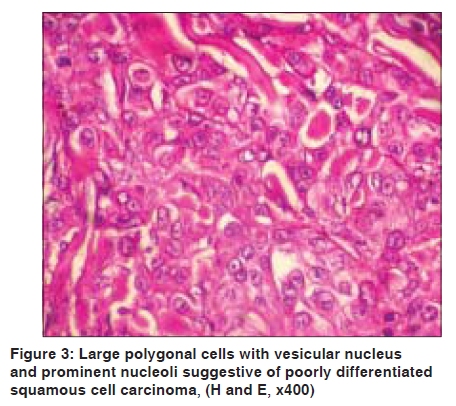
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 523-524 Letter to the Editor Keratoacanthoma like secondaries on the scalp V. Sreedevan, S. Pradeep Nair, G. Nanda Kumar1, Lissy Skaria, Rani Mathew, Anitha Sanker Department of Dermatology and Venereology, T.D. Medical College Alleppey and 1Department of Pathology, Medical College Trivandrum, Kerala, India Code Number: dv09173 PMID: 19736445 DOI: 10.4103/0378-6323.55411 Sir, Cutaneous manifestations of internal malignancy presents as paraneoplastic syndromes or as secondaries. Cutaneous metastases usually presents as multiple, discrete, painless, freely movable nodules of sudden onset, varying in color from red to bluish purple to light brown and may be the first sign of internal malignancy especially of the lung, kidney and ovaries. [1],[2] Lung carcinoma presenting with cutaneous metastases accounts for 4% of all cutaneous metastases. [3] A 48-year-old male presented with multiple well-defined discrete skin colored and erythematous 1.5-2.5 cm nodules distributed on the temporal, parietal and occipital region of the scalp of 2 months duration. Some of the nodules on the temporal and parietal region showed a central crater on its surface filled with keratin and crusts [Figure - 1]. The patient having suffered from a cerebrovascular accident 6 months ago and treated by indigenous medications was the only relevant past history. The patient was a chronic smoker using about 20 cigarettes per day for the past 15 years. CNS examination showed a left sided monoplegia. Respiratory system examination showed diminished breath sounds of right lung midzone. The only abnormality in the patient's routine laboratory investigations were a raised erythrocyte sedimentation rate (ESR) of 42 mm in first hr. Serological tests for syphilis, HIV-1 and 2 and hepatitis B and C were negative. Ultrasound abdomen did not show any lymphadenopathy or organomegaly. X-ray of the chest showed a homogenous opacity in the upper and midzone of right lung with a right basal pleural effusion. A contrast enhanced CT scan showed osteolytic lesions of the skull [Figure - 2], a mass of the right lung suggestive of bronchogenic carcinoma with multiple hyperechoeic areas in the mediastinal lymph nodes, brain and right kidney suggestive of secondaries. Skin biopsy of the nodule on the scalp showed a massive infiltrate of neoplastic large polygonal cells with prominent intercellular bridges, eosinophilic cytoplasm, pleomorphic vesicular nuclei with prominent nucleoli along with abnormal mitotic figures suggestive of poorly differentiated squamous cell carcinoma from bronchogenic carcinoma secondaries [Figure - 3]. A past history of chronic cigarette smoking, X-ray finding of homogenous opacity of right lung mid-zone, a CT scan finding of right bronchogenic carcinoma and histopathological finding of cutaneous infiltrates of poorly differentiated squamous cell carcinoma enabled us to make a final diagnosis of cutaneous secondaries on scalp from the lung primary. Since the morphology of nodules on the scalp resembled keratoacanthomas, we report this case as 'keratoacanthoma-like' secondaries on the scalp. Clinically squamous cell carcinoma and keratoacanthoma may mimic. Histopathology is the only diagnostic method even though keratoacanthoma may undergo spontaneous remission. Since the CT scan demonstrated multiple secondaries in the brain, mediastinal lymph nodes and right kidney, the most likely mode of metastases in this case including the scalp nodules is hematogenous. Cutaneous metastases indicates grade IV disseminated disease with poor prognosis and with death occurring within 3 months.[3] Hence it is of paramount importance to recognize cutaneous metastases as early as possible as they are often the first presentation of internal malignancy as our case demonstrates. The short duration of illness in our patient could be attributed to the fact that the histopathological finding was of a poorly differentiated squamous cell carcinoma which are highly aggressive in nature. Metastases to the scalp from lung carcinoma is very rare. Recurrent nodules on the scalp with ulceration from a lung primary has been reported in this journal.[4] To the best of our knowledge, keratoacanthoma like cutaneous secondaries on the scalp from a lung primary has not been described in literature, indicating that the skin is indeed the mirror of the body. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09173f3.jpg] [dv09173f1.jpg] [dv09173f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}