 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
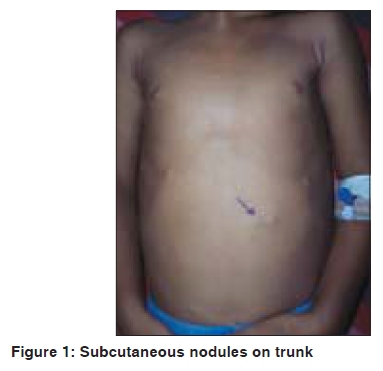
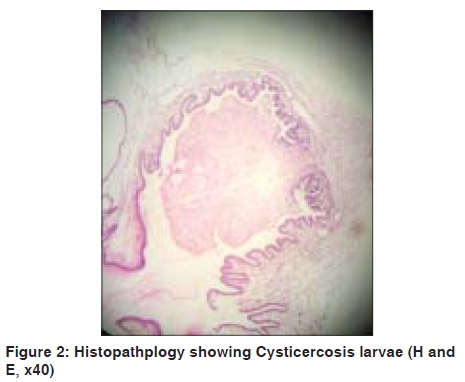
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 524-525 Letter to the Editor Neuro cysticercosis with subcutaneous nodules Sanjay Singrodia, R. G. Joshi, Rekha B. Solanki, Ranjan C. Rawal Department of Dermatology, Smt. N.H.L. Munici. Medical college, Vadilal Sarabhai General Hospital, Ahmedabad (Gujarat) India Code Number: dv09174 PMID: 19736446 DOI: 10.4103/0378-6323.55412 Sir, Cysticercosis is the most common parasitic infestation of the central nervous system, muscle and subcutaneous tissue, [1] caused by tissue-invading larval forms of the pork tapeworm, Taenia solium.[2] Central nervous system involvement is seen in 60-90% of patients with cysticercosis while 50-70% have epilepsy. [1],[2],[3] However, association of cysticercosis with subcutaneous nodules is not common. A five year-old female child was referred to the dermatology department with low-grade fever since the past five months and multiple swellings all over the body since two months. On examination, the patient was found to be febrile (100 o F) and pale. Multiple rounded, firm, nontender subcutaneous nodules of varying size (0.5-1 cm) were present on the scalp, back, abdomen and limbs [Figure - 1]. Two submucosal nodules were present on the left buccal mucosa. Systemic examination was within normal limits; fundus was normal. In the Paediatric ward, the patient was given oral antimalarials and antipyretics. On the 4 th day, she developed three episodes of seizures-the first episode was an unprovoked, left-sided seizure lasting for two minutes. She developed two more episodes of generalized, tonic-clonic seizure after 30 minutes. Parenteral phenytoin was started and maintained; there was no postictal neurological deficit. The hemogram was unremarkable except for a raised absolute eosinophil count (405/mm 3 ) and raised erythrocyte sedimentation rate (105 mm at one hour). The Mantoux test was negative and the antistreptolysin titre, C-reactive protein, antinuclear antibody and rheumatoid factor were all absent. Serum cholesterol levels, Renal function test and liver function test were all normal. Urine and stool examinations were normal and a perianal swab revealed no organisms. Chest X-ray, ultrasonography of the abdomen, and 2D-echo were normal. X-ray of the limbs revealed no soft tissue calcifications. Cerebrospinal fluid analysis was normal. A Computed tomography scan of the brain revealed multiple granulomas and vesicular stage of NCC.[3] Excision biopsy of the subcutaneous nodules was taken and histopathological examination showed cysticerci (larval stage of T. solium ) [Figure - 2]. The confirmed diagnosis was neurocysticercosis with cysticercosis cellulosae cutis. The patient was started on oral albendazole (10 mg/kg/day) and phenytoin (5 mg/kg/day). Oral prednisolone (1 mg/kg/day) was given for 15 days in a tapering manner. The patient was discharged after 15 days and advised to complete a 28 days' course of albendazole. On follow-up after two weeks, the patient was found to be afebrile and the subcutaneous nodules had reduced in size and number. The patient continued phenytoin (5 mg/kg/day) for three months. Cysticercosis is the most common parasitic disease of the central nervous system worldwide, but cysticercosis cutis has been reported much less frequently. Cutaneous parasitism by larval cestodes can take the form of subcutaneous nodules, [1] generating a clinical differential diagnosis of infundibular cyst, lipoma, neurofibroma, reactive lymph nodes, granular cell tumor as well as malignant tumors. Patients usually have multiple subcutaneous nodules, as in our case. Cysticercosis should be considered in cases of subcutaneous nodules occurring in individuals in or from endemic areas; even without signs of central nervous involvement. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09174f1.jpg] [dv09174f2.jpg] |
| |||||||||

{kind=link}
{kind=link}