 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
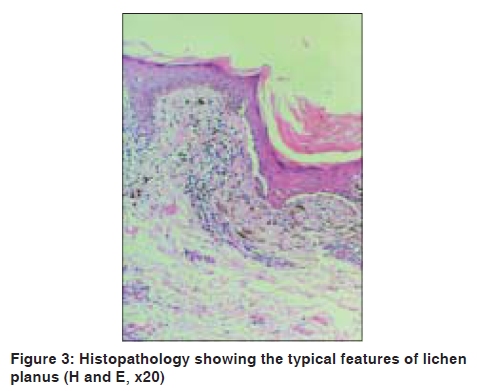
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 527-528 Letter to the Editor Lichen planus associated with imatinib mesylate Feroze Kaliyadan, T. S. Ganesan Departments of Dermatology and 1Oncology, Amrita Institute of Medical Sciences, Kochi, Kerala - 682028, India Code Number: dv09176 PMID: 19736448 DOI: 10.4103/0378-6323.55414 Sir, A 60-year-old male patient, a known case of chronic myeloid leukemia on imatinib came with pruritic skin rashes mainly over limb flexures and the abdomen, of three months duration. The patient had been on monotherapy with imatinib at the time of development of the rash for a period of 3 months. Subsequent to the withdrawal of the drug, for a period of two weeks, the rash started subsiding. The rash, however, recurred on restarting the drug. The patient did not give a history of any other significant skin or mucosal lesions. On cutaneous examination, well-defined violaceous papules and plaques were seen distributed mainly over the abdomen and the flexural aspect of both elbows and knees [Figure - 1] and [Figure - 2]. There was mild scaling but no evident vesiculation, oozing or crusting. The mucous membranes were uninvolved, so were the nails. The possibility of a lichenoid dermatitis/lichen planus induced by imatinib was considered. A skin biopsy was taken from the lesion; which was consistent with a diagnosis of lichen planus, (as opposed to lichenoid dermatitis) with no evidence of significant parakeratosis, spongiosis or eosinophilic infiltrate [Figure - 3]. The patient was started on topical steroids and antihistamines, following which there was significant improvement. Considering the importance of the drug (imatinib) in the treatment of the patient's leukemia, it was decided to continue the drug while simultaneously treating for the cutaneous lesions. The patient is at present being maintained on intermittent topical steroids (mometasone) and emollients. The patient has been on follow-up for the last three months and has shown excellent control of symptoms and signs. He has not reported any significant new lesions over the last three months. Imatinib has been reported to be associated with a number of cutaneous reaction patterns. In some series the incidence of cutaneous reactions has been reported to be as high as 69%. [1] Common cutaneous adverse effects include maculopapular eruptions and erythematous eruptions. Toxic epidermal necrolysis, Stevens-Johnson syndrome and acute generalized exanthematous pustulosis have also been reported with the use of imatinib. Other reported cutaneous adverse effects include: hypopigmentation, lichenoid reactions, pityriasiform eruptions, purpuric vasculitis, mycosis fungoides-like reactions, pityriasis rosea, psoriasis, reactivation or induction of porphyria cutanea tarda, neutrophilic eccrine hidradenitis, Sweet's syndrome and erythema nodosum. [1] Recently, there have been more reports of lichenoid dermatoses associated with imatinib. Various patterns have been reported including a chronic graft versus host type of lichenoid reaction, [2] lichen planus [3] and oral lichenoid dermatitis. [4],[5] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09176f3.jpg] [dv09176f2.jpg] [dv09176f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}