 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
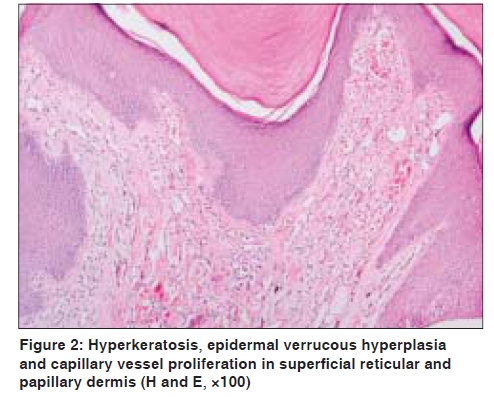
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 528-530 Letter to the Editor Verrucous hemangioma Ali Yaşar, Aylin Türel Ermertcan, Cemal Bilaç, Dilek Bayraktar Bilaç, Peyker Temiz1, Serap Öztürkcan Departments of Dermatology and 1Pathology, Celal Bayar University, Faculty of Medicine, Manisa, Turkey Code Number: dv09177 PMID: 19736449 DOI: 10.4103/0378-6323.55415 Sir, Verrucous hemangioma is an uncommon, congenital, localized, vascular malformation. Loria et al . defined this entity in 1958, and in 1967, Imperial and Helwig introduced the term 'verrucous hemangioma'. The lesion is generally noted at birth or in early childhood and is often located on the lower extremities. The early lesions are bluish-red in color; secondary infection is a frequent complication and this results in reactive papillomatosis and hyperkeratosis and thus the older lesions acquire a verrucous or warty surface. [1] Unlike other angiomatous nevi, they do not involute spontaneously. Clinically, they may resemble angiokeratoma, lymphangioma circumscriptum, verrucous epidermal nevus, verrucous cancer or even malignant melanoma. It can start as lesions resembling port-wine stains which may later become soft bluish-red vascular swellings that tend to grow in size and become verrucous. [2] A 22-year-old male patient presented to our outpatient clinic with a complaint of a verrucous lesion on his right foot since 15 years. Dermatological examination revealed a violet-colored verrucous plaque 4 × 2 cm in size on the right side of his right foot dorsum [Figure - 1]. Incisional skin biopsy was performed. Histopathological examination revealed hyperkeratosis, epidermal verrucous hyperplasia and capillary vessel proliferation in superficial reticular and papillary dermis [Figure - 2]. Diagnosis of verrucous hemangioma was made on clinical and histopathological examination. We referred our patient to a Plastic Surgery clinic. The lesion was totally excised . No recurrence has been observed during 8 months' follow-up period after surgical excision. A few atypical clinical presentation of verrucous hemangioma have been reported in the literature. Wentscher and Happle reported a 16-year-old male patient having multiple angiokeratotic lesions arranged in a linear pattern on his left arm. [3] Akyol et al . reported a 5-year-old boy with verrucous hemangioma in the glans penis and discussed briefly the hyperkeratotic vascular stains, which constitute a heterogenous group. [4] Histologically, verrucous hemangioma appears initially as a capillary hemangioma concentrated in the dermis and the hypodermis that later, after an intense proliferative reaction of the epidermis, adopts a verruciform pattern with hyperkeratosis, papillomatosis, irregular acanthosis, and an underlying capillary, cavernous, or mixed hemangioma in the dermis and subcutaneous tissue. The hemangiomatous component is greatly composed of dilated capillary and larger cavernous, endothelial-lined, blood-filled spaces. Inflammatory cells, hemosiderin, and fibrosis may be present in the upper dermis. The histopathological appearance closely resembles angiokeratoma as both lesions show vascular spaces just beneath a papillomatosis and hyperkeratotic epidermis. However, in contrast to angiokeratoma, the vascular spaces in verrucous hemangioma also involve the lower dermis and subcutaneous tissues. [1] Superficial ablative procedures like electrocautery, cryosurgery and laser application almost invariably lead to recurrence of the lesion. A combined approach using surgery and laser have been reported with good results. Yang and Ohara reported 14 patients presenting with small, localized lesions that were cured by one session of surgery without recurrence, while the 9 patients with wider and more extensive lesions required combination therapy in several stages for optimal results. [5] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09177f1.jpg] [dv09177f2.jpg] |
| |||||||||

{kind=link}
{kind=link}