 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
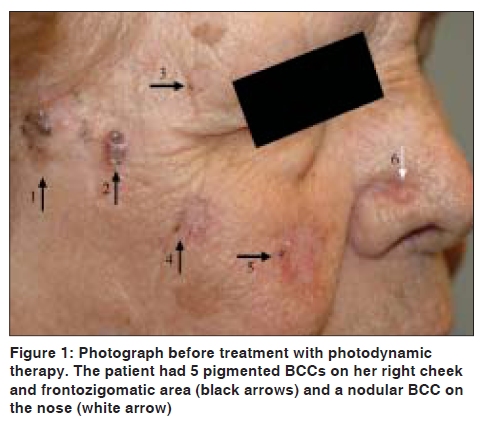
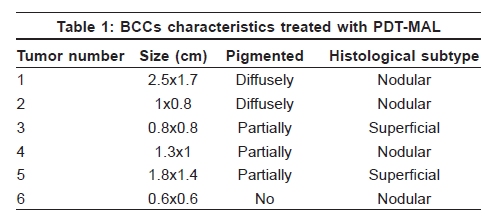
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 530-531 Letter to the Editor Pigmented basal cell carcinomas treated with photodynamic therapy José J. Pereyra-Rodríguez, José Bernabew-Wittel, Purificación Gacto-Sanchez1, Julián Conejo-Mir Departments of Dermatology, 1Plastic and Reconstructive Surgery, Virgen del Rocío University Hospitals, Sevilla. Spain Code Number: dv09178 DOI: 10.4103/0378-6323.55416 Sir, Basal cell carcinomas (BCC) are the most common malignancies among people with white skin. Overall pigmented BCCs are not very common, although its frequency can reach up to 20% of the total BCCs in people from the Mediterranean. [1] Photodynamic therapy (PDT) using methyl-aminolevulinate (MAL) is a treatment based on a phototoxic reaction that has proved to be successful for the eradication of superficial and nodular basal cell carcinoma as well as Bowen's disease with good cosmetic results [2],[3] including large Phase III studies of MAL-PDT. [4] PDT is not recommended for pigmented BCC because it is generally thought that pigments might cause difficult light absorption into tumoral cells. [5] However, the effectiveness of PDT in pigmented BCC has not been properly studied. We report five cases of pigmented BCC treated with PDT-MAL with complete clinical response. A 79-year-old female with multiple BCCs was treated during the earlier years in our department with cryotherapy, topical 5% imiquimod, and excisional surgery. She was referred again to us with 6 new tumoral lesions on her face [Figure - 1]. Because the patient refused surgery, cryotherapy or topical 5% imiquimod, PDT was proposed to her as a palliative treatment. After her written consent, PDT was performed. A histopathological examination confirmed five pigmented BCCs located on her right cheek and zigomatic area and 1 non-pigmented nodular BCC on her nose [Table - 1]. Before administration, 160 mg/g of MAL cream (Metvix® , Galderma) was applied to the lesions in order to facilitate access of MAL to all parts of the lesion. The extent of preparation was dependent on the nature of the lesion. Superficial lesions were debrided with a curette to remove scales and crusts. The lesion surface was scraped gently in order to increase penetration of the active agent. Intact skin covering nodular lesions was removed by shaving the lesion over the tumour margins. MAL 160 mg/g cream was applied, approximately 1 mm thick, on the lesion and 10 mm on the surrounding skin. After application of the cream, the lesion area was covered by an adhesive and occlusive dressing for 3 hours. When the occlusive dressing was removed, the remaining cream was gently cleaned off using saline. The lesione area was then illuminated using a light source Aktilite® 37 J/cm 2 . Time of exposure was automatically calculated by the light source (9 minutes per session). Lesions were covered with a light protective dressing after treatment for a full day. The treatment cycle was repeated once 1 week later. Lesion responses were evaluated clinically after 2 months. All treated lesions showed a complete clinical response. The patient refused a histological confirmation but 1 year later there were no signs of recurrence [Figure - 2]. It is well-known that the gold standard treatment for BCCs is surgery. [6] Micrographic Mohs surgery must be reserved only for certain histological subtypes.[6] However, other modalities of treatment such as cryotherapy, electrodesiccation, and curettage have been used with a wide ranges of success. Certain cases, such as large and multiple lesions located in difficult scarring areas, systemic risk factors that contraindicate surgery, and patients that refuse surgery, constitute a challenge for dermatologists. [2] The existence of pigments is classically considered one criteria of exclusion for PDT, because in those particular cases the light penetration into the skin is considerably reduced. [5] However, no scientific evidence supporting this argument was found. In our experience, pigmented BCCs treated by PDT-MAL demonstrated a high rate of complete regressions, in the same pattern of the non-pigmented lesions. We need to point out the importance of an adequate debulking prior to PDT-MAL, which is possibly the reason why it was previously not considered as an alternative treatment. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09178f1.jpg] [dv09178t1.jpg] [dv09178f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}