 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
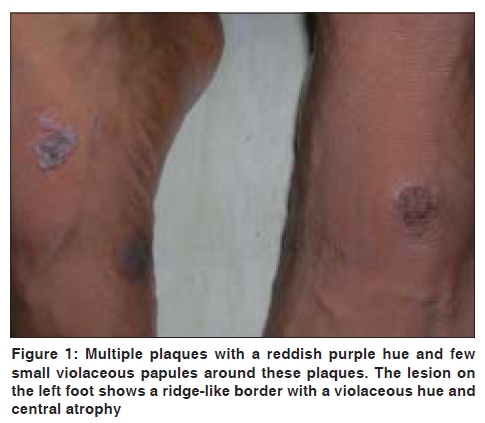
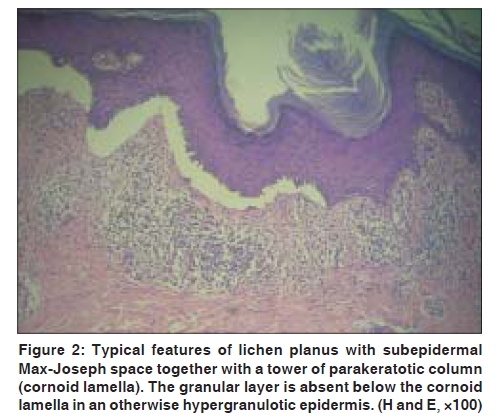
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 532-534 Letter to the Editor Co-localization of lichen planus and porokeratosis of Mibelli Sudip Kumar Ghosh, Debabrata Bandyopadhyay, Gobinda Chatterjee, Arghya Prasun Ghosh Department of Dermatology, Venereology and Leprosy, R.G. Kar Medical College, Kolkata, India Code Number: dv09180 PMID: 19736452 DOI: 10.4103/0378-6323.55418 Sir, Coexistence of lichen planus (LP) with a number of dermatological disorders is well documented. We are reporting here a case of co-localization of lichen planus with porokeratosis of Mibelli in a 40-year-old man who presented with some itchy bluish-black lesions on the dorsum of his feet for one year. The patient recalled having some brownish, circular, asymptomatic spots on his feet since childhood. He noticed that over the last few months the spots had been gradually increasing in size and became elevated and itchy. In addition, a few pigmented, itchy, small elevations appeared in the vicinity of the preexisting lesion on the right foot. There was no family history of similar lesions and no history of any drug intake prior to the exacerbation of eruptions. Cutaneous examination showed multiple dark brown plaques with a reddish purple hue at some areas and a few small violaceous papules around these plaques. They were distributed over dorsum of both feet and over ankles. Close examination of a plaque on the dorsum of left foot showed an elevated ridge-like border with central groove surrounding an atrophic area, the border at places showing some broadening with a distinct violaceous color [Figure - 1]. The nails, oral mucosae and other parts of skin were free from any lesion. Two 4-mm punch biopsies from the elevated borders of plaques on dorsum of both feet showed a similar but distinctive picture. There was ortho-hyperkeratosis with irregular saw tooth-like elongation of rete ridges and a few towers of parakeratotic columns invaginating into the epidermis, beneath which there was absence of granular layer (comprising the so-called cornoid lamellae). Focal hypergranulosis, basal cell degeneration at some areas and melanin incontinence were also seen. Just beneath the epidermis, there was a lymphohistiocytic infiltrate in a band-like fashion, which extended laterally beyond the cornoid lamellae. Subepidermal clefts (Max Joseph's spaces) were also noted in some areas [Figure - 2]. A direct immunofluorescence examination could not be done due to economic constraints and local non-availability. Histopathologically, lichen planus is characterized by hypergranulosis, irregular acanthosis, basal cell degeneration, melanin incontinence and subepidermal clefts, known as Max Joseph's spaces. In LP, parakeratosis is conspicuous by its absence, [1] while the histopathological hallmark common to all types of porokeratosis is the cornoid lamella, which consists of tightly packed columns of parakeratotic cells surrounded entirely by orthokeratotic stratum corneum. Agranulosis is found below the cornoid lamella. [5] In the center of the lesion, epidermis is usually atrophic with flattening of rete ridges and areas of basal cell degeneration. The co-localization of skin diseases remains one of the most elusive problems in dermatology. Co-localization of LP have been described with subacute cutaneous lupus erythematosus, generalized morphea, lichen sclerosus, [2] generalized lichen amyloidosis, [3] Riehl's melanosis, [4] psoriasis and vitiligo. [6] An association of four distinct disorders, namely, lichen planus, vitiligo, lichen sclerosus and disseminated actinic porokeratosis has also been reported in a 70-year-old man. [7] In our patient, typical plaques of porokeratosis as well as LP was clinically evident. In addition, some porokeratotic plaques clinically showed lichen planus-like morphology particularly along borders that showed distinctive histologic features of both lichen planus and porokeratosis in the same microscopic fields. Although Nekam's disease (keratosis lichenoides chronica) may show a lichenoid histology underneath a parakeratotic epidermis and may rarely be associated with porokeratosis, [8] this diagnosis was not considered owing to the lack of typical clinical features and histology of this condition. Authentic clinical and histologic features of Nekam's disease are, respectively, [9] a facial seborrheic dermatitis-like eruption with tiny confluent papules on the trunk and extremities in linear and reticulate arrays and an infundibulocentric and acrosyringocentric lichenoid interface dermatitis with numerous necrotic keratocytes covered by parakeratosis housing neutrophils in staggered fashion. The history of the present case suggests that the patient might have had porokeratosis since his childhood and he probably became symptomatic as he developed lichen planus on and around the porokeratotic plaques. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09180f2.jpg] [dv09180f1.jpg] |
| |||||||||

{kind=link}
{kind=link}