 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
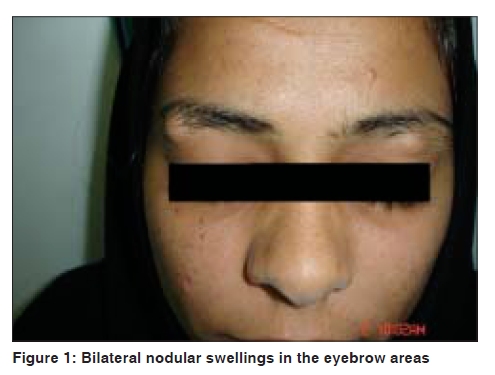
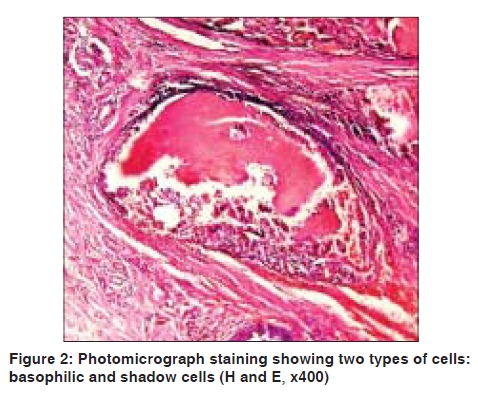
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 535-537 Letter to the Editor Bilateral pilomatricomas of the brow region in a female Fatemeh Shafikhani, Sarah Hashemzadeh, Arash Ayoubi Department of Dermatology of Imam Khomeini hospital, Jondi Shapur medical university of Ahwaz, Iran Code Number: dv09182 PMID: 19736454 DOI: 10.4103/0378-6323.55420 Sir, Here, we report a case of bilateral pilomatricoma of the brow region. We believe that this case is unique because of the bilateral involvement of this area. Multiple pilomatricomas are rare and are mostly associated with other conditions. [1],[2],[3],[4] This case did not have any associations. The patient is a 20-year-old female who presented with bilateral nodules of the brows since the last 1 year. The right nodule was 1.5 x 1 cm and the left nodule was 1 x 1 cm in size [Figure - 1]. They were firm on consistency but were mobile on the underlying structures. The overlying skin was normal in appearance. Her family history for the same condition was negative. She did not report any other disorder or any history of trauma. Routine laboratory tests were normal. The clinical differential diagnosis included epidermal cysts, pilar cysts and pilomatricomas. Fine needle aspiration was performed but no aspirate was achieved. Total excision of one of the nodules was performed. Histopathologic evaluation revealed irregularly shaped islands of epithelial cells. Two types of cells, basophilic cells and shadow cells, comprised the islands [Figure - 2]. Thus, the diagnosis of pilomatricoma was confirmed. Excision of the other nodule showed the same changes. Pilomatricomas arise from the hair follicle matrix cells. This tumor makes up around 20% of all hair follicle-related tumors. The majority of the patients are under 20 years of age, and females are affected more often than males. [1] The tumor presents as a solitary, firm, painless, dermal or subcutaneous mass. It slides freely over the underlying tissue and the overlying skin has a reddish or blue hue in about 24% of the patients. On stretching the overlying skin, it may show the "tent sign" with multiple facets and angles. Pilomatricoma most commonly occurs in the head and neck, with cervical, temporal, eyelid and preauricular regions being the most frequently reported locations. Growth is usually slow and benign. The tumor diameter ranges from 0.5 to 3 cm. A malignant variant with distant metastases has been described. [2],[3] Pilomatricomas are generally solitary tumors; multiple tumors occurring synchronously account for 2-3.5% of those reported. Multiple or recurring tumors may be found in association with Gardner syndrome, myotonic muscular dystrophy, sarcoidosis, skull dysostosis, Rubenstein-Taybi syndrome and Turner syndrome. [2] The pilomatricoma lesions rarely develop simultaneously. Instead, they have a tendency to develop in intervals of one to several years. [2],[3] In the differential diagnosis, it may be necessary to rule out midline dermoid cysts in the neck, parotid tumors in the preauricular region and adenopathy, calcified hematoma and lipoma in other sites. Pilomatricoma should be differentiated from epidermal and dermoid cysts. [2] Histopathologically, the tumor is sharply demarcated. Embedded in a rather cellular stroma, irregularly shaped islands of epithelial cells are present. As a rule, two types of cells, basophilic cells and shadow cells, comprise the islands. [4] Shadow cells are enucleated and are formed by keratinization of the basaloid cells, which decrease in number as the neoplasm ages. [2] With the von Kossa stain, calcium deposits are found in approximately 75% of the tumors. Areas of ossification are seen in 15-20% of the cases. Sometimes, melanin deposition and transepidermal elimination have also been described. [4] For definitive diagnosis and because spontaneous regression is never observed, complete surgical excision is the treatment of choice. [2] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09182f1.jpg] [dv09182f2.jpg] |
| |||||||||

{kind=link}
{kind=link}