 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
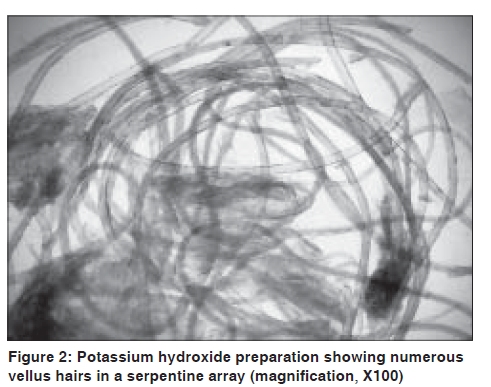
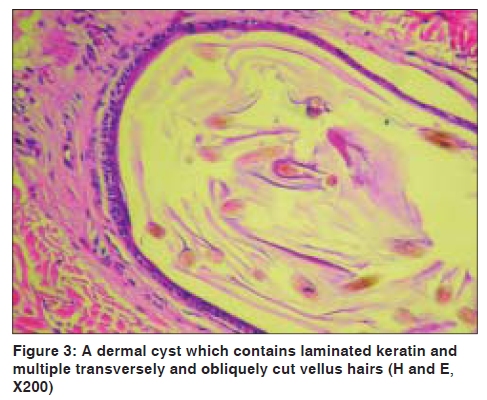
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 537-538 Letter to the Editor Eruptive vellus hair cysts: An alternative diagnosing method Ayse Serap Karadag, Ebru Cakir1, Aylin Pelitli Department of Dermatology, Ankara Kecioren Research and Training Hospital, 1Department of Pathology, Atatürk Chest Diseases and Thoracic Surgery Centre, Ankara, Turkey Code Number: dv09183 PMID: 19736455 DOI: 10.4103/0378-6323.55421 Sir, Eruptive vellus hair cysts (EVHC) are unusual developmental abnormality of vellus hair follicles. [1] Diagnosis is generally made by clinical presentation and confirmed with punch biopsy and histological examination. Recently minimally painful or painless, nonscarring techniques have been described. [2] We report a 10-year-old girl diagnosed as EVHC with an alternative method. A 10-year-old girl presented with generalized papular eruption. The skin lesions initially appeared on anterior chest two years ago and then spread to upper and lower extremities. The number of lesions gradually increased. She had no subjective symptoms. Her past medical and family history was unremarkable. Dermatological examination revealed multiple, smooth, soft, fresh colored, 1 to 3 mm, follicular papules on the anterior chest, upper and lower extremities [Figure - 1]. The rest of her cutaneous examination was within normal limits. The clinical diagnosis of EVHC was made. The cysts were relatively superficial and therefore we attempted an alternative method to support the diagnosis. After local application of anesthetic cream containing lidocaine and prilocaine (EMLA® cream, Astra-Zeneca, Turkey) for an hour; a tiny incision was performed on the top of a lesion and cystic material was gently squeezed. Microscopic examination of the cystic material in a 10% potassium hydroxide preparation demonstrated numerous vellus hairs [Figure - 2]. A skin punch biopsy was performed to confirm the diagnosis. Histopathological findings demonstrated a cystic structure lined by squamous epithelium in the lower dermis. Vellus hairs and laminated keratinous materials were present within the cyst; no sebaceous structure was seen within the cyst wall [Figure - 3]. These findings were consistent with EVHC. The patient refused the mechanical treatment option so she was treated with topical tretinoin. There was no evidence of clinical improvement even after two months of the treatment. EVHC presents on the chest and extensor or flexor surfaces of the extremities. The lesions have been described as skin colored macules or papules, ranging in size from 1 to 5 mm and numbering from 20 to 200. EVHC may be sporadic or be inherited in an autosomal dominant manner. [1],[2] The clinical differential diagnosis includes steatocystoma multiplex, trichilemmal and dermoid cysts, comedones of acne, keratosis pilaris, perforating disorders, folliculitis, syringomas, milia, and molluscum contagiosum. [1],[3] Trichostasis spinulosa (TSS) is another important disorder in the differential diagnosis of EVHC. Protruding vellus cysts in TSS may be inapparent to naked eyes and the disease may clinically simulate EVHC. [4] Histological examination is essential to differentiate these similar skin lesions. [5] Clinical presentation is usually diagnostic for EVHC but sometimes the diagnosis should be confirmed with punch biopsy and histological examination. Nevertheless, punch biopsy can be both distressing and painful, and may leave an unpleasant scar. [2] In the present case, we used an alternative method to support the clinical diagnosis. A similar technique was reported by Sardy and Karpati. The author utilized a sterile, large (18 Gx2) blood-collecting needle to aspirate cystic contents from anesthetized skin. [3] Recently Kaya et al. [5] reported a different technique, which is also used for treatment. After puncturing the overlying skin using the sharp-tipped cautery point, they grasped the base of the cyst using a standard dissecting forceps and they extracted the cysts out. [5] These techniques are less invasive methods than punch biopsy. EVHC are usually asymptomatic lesions but treatment is necessary for cosmetic reasons. Spontaneous resolution can be seen in one-fourth of the patients because of transepidermal elimination. Topical (retinoic acid, 12% lactic acid, 10% urea), mechanical (cauterization, curettage, dermabrasion, CO 2 laser) and systemic (oral isotretinoin) treatment modalities are available. [1],[5] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09183f1.jpg] [dv09183f2.jpg] [dv09183f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}