 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
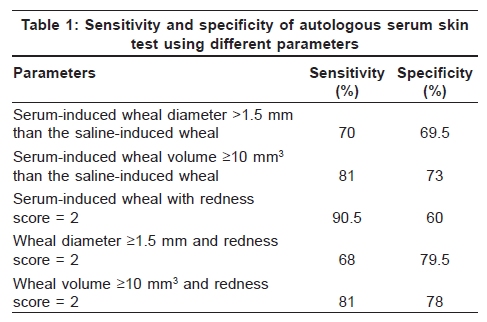
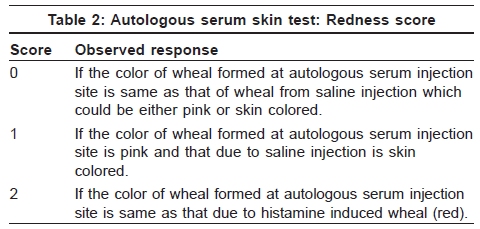
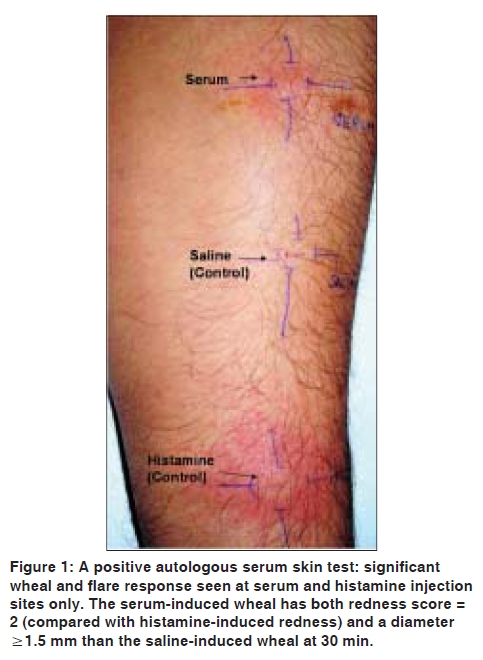
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 545-548 Resident's Corner Autologous serum skin test: Methodology, interpretation and clinical applications Surbhi Vohra, Nand Lal Sharma, Vikram K. Mahajan Department of Dermatology, Venereology and Leprosy, Indira Gandhi Medical College, Shimla, India Code Number: dv09186 PMID: 19736458 DOI: 10.4103/0378-6323.55424 Introduction Autoimmune urticaria, a recently described subset of chronic urticaria, has often severe and continuous whealing associated with malaise, indigestion and sensation of hot and cold. A personal or family history of other autoimmune diseases or urticaria in family members is suggestive. It is associated with antithyroid antibodies in 27% of patients or with other autoimmune conditions such as vitiligo, rheumatoid arthritis, pernicious anemia and insulin-dependent diabetes mellitus. [1],[2] Diagnosing these patients becomes important as they need high doses of antihistamines and systemic corticosteroids during acute exacerbations. Immunomodulatory drugs, while their use is not justified in chronic idiopathic urticaria (except in antihistamine refractory chronic urticaria cases), are therapeutic benefit in recalcitrant to therapy autoimmune urticaria patients having significantly impaired quality of life. [3] Immunologically, it is characterized by the presence of functional autoantibodies that activate mast cells and basophils by crosslinking the high-affinity IgE receptor (FceRI). About 50% patients of chronic urticaria have functional autoantibodies to FceRI and 9% to the IgE antibody itself. [4],[5] Autoimmune urticaria is thus diagnosed in ASST-positive chronic urticaria patients who exhibit functional autoantibodies against IgE and/or its high-affinity receptor FceRI. However, it is often clinically difficult to distinguish chronic urticaria from autoimmune urticaria. Its diagnosis is practically relied upon clinical suspicion and autologous serum skin test (ASST) as facilities for assaying functional histamine release from basophils or mast cells, a suitable diagnostic laboratory investigation, are largely confined to research centers. Unfortunately, the immunoblot assays, for binding of autoantibody to autoantigen, have not shown any correlation with basophil histamine release and attempts to develop a suitable enzyme-linked immunosorbent assay (ELISA) for clinical use to differentiate between functional and nonfunctional autoantibodies too has remained unsuccessful. Therefore, it becomes imperative for all practising dermatologists to know the precise methodology, accurate interpretation and clinical applications of ASST for effective management of autoimmune urticaria patients. Methodology Historically, in 1986, Grattan et al. [6] were the first to use ASST to differentiate autoimmune urticaria from chronic idiopathic urticaria. They injected intradermally 0.1 ml of autologous serum and normal saline as control in 12 patients of chronic idiopathic urticaria. The positive results were arbitrarily defined as formation of a wheal by serum within 2 h of injection that is at least 5 mm larger than that resulting from saline control and had a difference of 10 mm in the diameter of surrounding erythema. They observed positive responses in 7 patients within 30 min which attained their zenith in 90-120 min and remained positive for an average of 8 h. Subsequently, Sabroe et al. [7] standardized its methodology and defined the parameters which provide optimum sensitivity and specificity for detecting patients of chronic urticaria with autoantibodies [Table - 1]. [4] There have been numerous modifications in the methodology and interpretation of ASST since then in various studies. O'Donnell et al. [8],[9] from their two separate studies interpreted positive ASST as the mean diameter of serum-induced wheal being at least 2 mm larger than that of saline-induced wheal at 30 min. Bakos and Hillander [10] used 0.1 ml instead of 0.05 ml each of serum, histamine and saline. Toubi et al. [11] also used 0.1 ml of sterile autologous serum and determined the wheal/flare size at 30 min and followed up for 60 min and graded the responsed from 0 to +3 of ASST by measuring wheal/flare diameter as 0 = negative control; +1 = wheal 1.5 mm > negative control, flare 15 mm; +2 = wheal 3-5 mm > negative control, flare > 15 mm; +3 = wheal 6-10 mm > negative control. As ASST results tend to get modified with treatment, the patients should be off antihistamines for at least 2-3 days (long-acting antihistamine for 7 days) and doxepin for 2 weeks prior to the test to avoid false negative results. [7],[12],[13] Most studies also exclude patients taking corticosteroids or immunosuppressive agents during the foregoing 6 weeks to 3 months of ASST.[7],[14] In other words, the patient should have active disease at the time of ASST. However, the test is not performed over areas involved by wheals in the last 24 h. Preparation of Autologous Serum and Control Two milliliters of patient's venous blood is collected in a sterile glass tube and allowed to clot for 30 min at room temperature. The serum is then separated by centrifugation at 500× g for 15 min and used immediately for ASST. [12],[13] Histamine diphosphate 10 µg/ml for positive control and sterile physiological saline (0.9%) for negative control are used. [12],[13] Procedure and Interpretation Approximately 0.05 ml (equivalent to 2 units on insulin syringe that has 1 ml marked as 40 units) each of autologous serum, histamine diphosphate and sterile physiological saline is injected separately intradermally over volar aspect of the left forearm.[1],[4],[12],[15] Every time a separate syringe should be used for each solution. Autologous serum is injected most proximally and histamine more distally with normal saline in the middle keeping a gap of at least 5 cm between the two injection sites. After 30 min (15 min for histamine), the wheal formed at each injection site is measured at two perpendicular diameters (d 1 and d 2 ) and the average of the two is calculated. [1],[4],[12],[15] Wheal area can also be calculated according to the formula ð [(d1 +d 2 ) 2 /4].[2] If needed the wheal volume can be calculated by multiplying the wheal area by half the change in skin-fold thickness measured with a low-tension spring-loaded thickness measuring gauge. The surrounding flare is often ignored but the redness response is measured as ' redness score ' [Table - 2]. [4] Positive ASST is the one with serum-induced wheal which has both redness score = 2 and a diameter (average of d 1 and d 2 ) of ≥1.5 mm as compared to the saline-induced wheal at 30 min [Figure - 1]. Using this criterion, the sensitivity and specificity of the ASST for detecting autoantibodies is 70 and 80%, respectively, and false positive results in healthy subjects and controls are minimal. Clinical Relevance The reported prevalence of ASST positivity in patients of chronic urticaria varies from 35 to 58% in various studies. [6],[8],[9],[10],[16] Autologous serum skin test (ASST) positivity has been found to correlate well with the severity and duration of attacks of urticaria. [11],[17] However, it needs to be kept in mind that positive ASST does not specifically imply mast cell degranulation by autoimmune stimulation as a cause of the wheal response. It rather helps to define a subgroup of patients with chronic urticaria who are most likely to have endogenous cause and the results must be interpreted in the context of clinical relevance. Comments Despite being the most accessible and useful test for demonstrating endogenous vasoactive factors in the patient's blood with chronic idiopathic urticaria, a positive ASST is not synonymous to autoimmune urticaria. The significance of a negative ASST also remains less clear. For instance, the reported prevalence of positive ASST in chronic urticaria is about 60% while IgG antibodies specific for the high-affinity IgE receptor FceRI or IgE are detected in not more than 30−40% of ASST-positive patients. [18] This signifies that different histamine-releasing factors, some chemokine-like, may be involved in vivo, and that such factors may also be clinically relevant in ASST-negative patients. Validity of ASST also remains questionable in view of the findings of a recent study by Bajaj et al ., [19] wherein they used autologous serum therapy in ASST-positive and ASST-negative chronic urticaria patients and could prevent relapse almost equally well in both the groups for as long as 2 years suggesting existence of a subset of ASST-negative autoimmune urticaria patients. They suggested that the ASST positivity perhaps reflects an autoreactive state to multiple and yet to be identified circulating factors in the patient's own blood. It is probable that the ASST-negative patients possess a different IgG subclass with decreased ability to release histamine from basophil activation. Although all these may partly be explained on the basis of results being false negative in ASST-negative autoimmune urticaria patients, future studies may unravel these aspects. Autologous serum skin test (ASST) is also not bereft of limitations. Although it may not hold true in all cases, a positive ASST has been demonstrated to be associated with the presence of H. pylori antibodies. [14],[20] Interestingly its reactivity also correlates strongly in patients who have multiple intolerances to nonsteroidal antiinflammatory drugs. [21] It is time-consuming, needs expertise for reproducibility, stopping antihistamines prior to the test in severe cases may be difficult, testing over the site of recent wheals may alter the results and the results may sometimes need to be correlated with in vitro basophil histamine-release assays. [4],[5] There are also health and safety issues involved in relation to the preparation of autologous serum. Nevertheless, ASST offers a simple screening test for potentially relevant biological activity and may help to define a subgroup of patients with urticaria who are more likely to have an endogenous cause for their disease than do patients without a positive test. It has good sensitivity and even better sensitivity in detecting autoantibodies in children as well. [22] Therefore, it can reasonably be used as a predictive clinical test to diagnose autoimmune urticaria, especially in situations where the basophil histamine-releasing test is not available. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09186t1.jpg] [dv09186t2.jpg] [dv09186f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}