 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
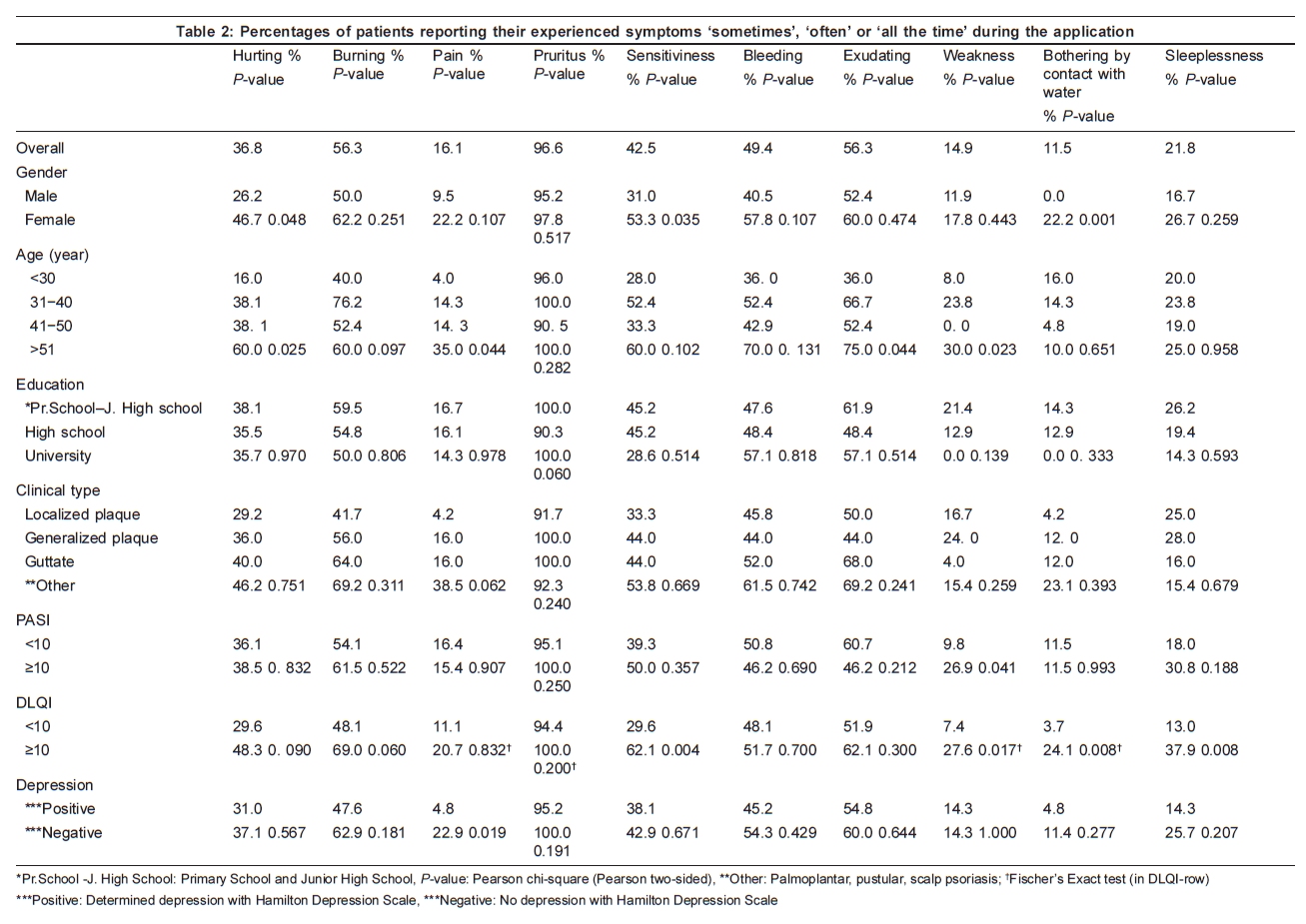
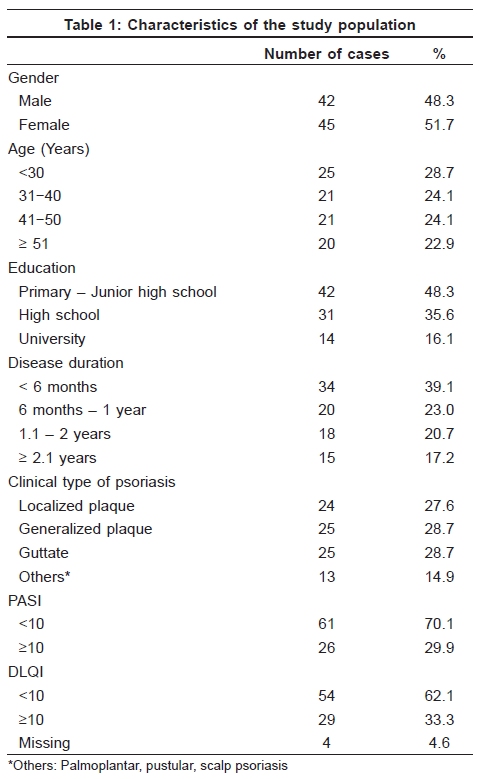
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 551 Net Study The relationship between symptoms and patient characteristics among psoriasis patients Cemal Bilaç, Aylin Türel Ermertcan, Dilek Bayraktar Bilaç, Artuner Deveci1, Gönül Dinç Horasan2 Celal Bayar University, Faculty of Medicine, Departments of Dermatology, 1Psychiatry and 2Public Health, MANİSA. Code Number: dv09188 PMID: 19736461 DOI: 10.4103/0378-6323.55426 Abstract Background: Pruritus is a common symptom of many dermatological and systemic diseases. It is a common complaint among patients with psoriasis of the chronic plaque type. Patients with pruritus suffer from more severe psoriasis although some authors did not find a significant relationship between pruritus intensity and psoriasis severity.Aims: In this study, we aimed to investigate the relationship between clinical features and symptoms among psoriasis patients. And also we aimed to evaluate whether the severity of disease, depression and quality of life scores could effect these symptoms or not. Methods: Eighty seven patients with psoriasis were enrolled in this study. Epidemiological data of patients were noted. Clinical symptoms, such as pruritus, pain, burning, exudation, bleeding, weakness, etc. were interrogated. The answers to these questions were classified as 'never', 'rare', 'sometimes', 'often' and 'all the time'. Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index (DLQI), Hamilton Anxiety-Depression Scale (HAD) were calculated for each patient. PASI and DLQI scores were classified as ≥ and <10. Results: We found that the most frequent symptom was pruritus (96.6%). Other frequent symptoms were burning (56.3%), exudation (56.3%) and bleeding (49.4%). Hurting, sensitiveness and bothering were more frequent in women. Percentages of hurting, pain, exudation and weakness symptoms had been increasing with age. Frequency of weakness was significantly high in PASI ≥ 10 patients. Conclusion: Pruritus is a very common symptom in psoriasis. Burning, exudation and bleeding are also common symptoms seen in psoriasis. New scoring systems including symptoms of psoriasis patients may be developed for evaluating the severity of the disease. Keywords: Psoriasis, Symptom, Sign, Severity Introduction Psoriasis is one of the most common chronic inflammatory skin diseases with a complex, multifactorial and still not fully understood etiopathogenesis. [1] It is estimated that approximately 1-2% of the general population of highly developed countries has psoriasis. [2] Pruritus is a common symptom of many dermatological as well as systemic diseases. It is a common complaint among patients with psoriasis of the chronic plaque type.[1],[2] Prevalence of pruritus in psoriasis has been reported from different parts of the world ranging from 64-84%.[3] The main dermatology textbooks describe only in passing pruritus in psoriasis and rarely mention other symptoms. [4] Patients with pruritus suffer from more severe psoriasis, although some authors did not find a significant relationship between pruritus intensity and psoriasis severity. The presence and intensity of itching has been found to be independent of age, gender, marital status, family history of psoriasis or atopy, type of psoriasis, alcohol or smoking habits, duration of the disease, as well as duration of the last outbreak of psoriasis. [1] Some textbooks report that itching is an uncommon complication of the disease, induced by topical therapy or depending on the emotional state of the patient. On the other hand, a few studies performed to evaluate pruritus in psoriatic patients found a high prevalence of this symptom, with estimates ranging from 67 to 92%, also depending on what was actually measured (i.e. presence/absence, frequency, intensity). Nevertheless, in clinical practice it is known that in patients with psoriasis 'the skin may itch, burn, sting, and bleed easily in affected areas'. [4] Pain was another associated symptom and was reported by 17% of pruritic patients; this has rarely been reported in pruritus. [5] The only symptom which is at times considered is itching, whereas pain, burning or bleeding are mentioned even more rarely. [4] In this study, we aimed to evaluate the associations between pruritus, other clinical symptoms and patient characteristics in psoriasis patients. And also we aimed to investigate whether the severity of psoriasis, depression and Dermatology Life Quality Index (DLQI) scores have effects on these symptoms or not. Methods Eighty-seven patients with psoriasis composed of 42 (48.3%) male and 45 (51.7%) female patients were enrolled in this study. Patients having other dermatological or systemic diseases were excluded from the study. Psoriasis patients were classified as localized plaque, generalized plaque, guttate, palmoplantar, pustular and scalp psoriasis according to the clinical types. Palmoplantar, pustular and scalp forms of psoriasis were grouped in the 'other' category due to the few number of these patients. The severity of disease was calculated according to 'Psoriasis Area and Severity Index (PASI)'. Dermatology Life Quality Index (DLQI) and Hamilton Anxiety−Depression (HAD) scores were calculated for each patient. PASI and DLQI scores were classified as ≥ and < 10. The patients were also classified as having 'presence of depression' and 'absence of depression' according to HAD scale. We analysed the symptoms by asking for the presence of hurting, burning, pain, pruritus, sensitiveness, bleeding, exudation, weakness, botheration by contact with water and sleeplessness. Patients answered the presence of symptoms by 'never', 'rarely', 'sometimes', 'often' or 'all the time'. Presence of symptoms were transformed into a dichotomous variable; patients who answered 'sometimes', 'often' or 'all the time', as 'cases' for each symptom while patients answering 'never' or 'rarely' were considered as 'noncases'. We analyzed the prevalence of each symptom in subgroups of the study population determined by gender, age, education level, clinical type of psoriasis, state of depression, PASI and DLQI scores [Table - 2]. Statistical analysis Comparisons between the presence of clinical symptoms and clinical and sociodemographic variables were performed with the Pearson Chi-square test and Fischer's exact test. ' p < 0.05' was considered statistically significant. All statistical analyses were performed with SPSS, version 10.0 for Windows. Results A total of 87 patients (42 male, 48.3% and 45 females, 51.7%) with psoriasis were included in the study. Patients' ages ranged between 16 and 81 and the mean age was 39.5 ± 15. Duration of the disease ranged between 1 and 40 months (mean 12.4 ± 9.9). When we look at the clinical types of psoriasis, the percentages were 27.6, 28.7, 28.7 and 14.9% for localized plaque, generalized plaque, guttate and others, respectively. PASI scores of patients were < 10 in 61 patients (70.1%) and ≥10 in 26 patients (29.9%). DLQI scores were < 10 in 54 patients (62.1%) and ≥10 in 29 patients (33.3%). The characteristics of the study population are presented in [Table - 1]. Pruritus was the most frequent symptom in psoriasis patients (96.6%). Burning (56.3%), exudation (56.3%) and bleeding (49.4%) ensued pruritus as more frequent symptoms in patients. 'Botheration by contact with water' was found to be the rarest symptom (11.1%). The frequency of hurting, sensitiveness and weakness were higher in women than in men (Pearson's Chi-square test, p < 0.05). More frequent symptoms other than pruritus were burning and exudation in males and females respectively. Interestingly, we did not determine 'botheration by contact with water' symptom in male patients. Hurting, pain, exudation and weakness were more often observed in older patients (except absence of weakness in 41-50 years of ages). We did not observe association between symptoms and education level or clinical type of psoriasis. Although more frequent symptoms other than pruritus were exudation (50.0%) and bleeding (45.8%) in localized plaque type, burning (56.0%) was in generalized plaque type, exudation (68.0%) and burning (64.0%) were in guttate and other types of psoriasis. Only 'weakness' symptom was found to be significantly higher in PASI ≥ 10 patients ( p = 0.041). The frequency of other symptoms were higher (hurting, burning, pruritus, sensitiveness, sleeplessness), equal (bothering by contact with water) or less (pain, bleeding, exudation) in PASI ≥ 10 patients. The frequency of all symptoms were higher in DLQI ≥ 10 patients. Sensitiveness ( p = 0.004), weakness ( p = 0.017) and botheration by contact with water ( p = 0.008) were found to be significantly high in these patients. Pain was found to be statistically higher in the presence of depression as determined by HAD scale ( p = 0.019). Also, all the other symptoms (except weakness) were found to be higher in depressive psoriatic patients than in nondepressive ones. Discussion Even though in clinical practice it is known that 'the skin may itch, burn, sting, and bleed easily in affected areas' in patients with psoriasis, there are a few studies evaluating the frequency of these symptoms, except pruritus. [4] To the best of our knowledge, the prevalence of bleeding and burning has rarely been reported. [6] Prevalence of pruritus in psoriasis, ranging from 63 to 84%, has been reported from different parts of the world. Despite a high prevalence of pruritus in psoriasis, limited information is available on this subject. Pruritus is more common in plaque-type psoriasis compared with other types of psoriasis such as guttate, pustular or erythrodermic. Characteristics of pruritus in psoriasis are not well documented. [3] A study performed by Sampogna et al . suggested that two-thirds of patients experienced itching often or all the time during 4 weeks before admission. Moreover, 26% of patients reported that their skin hurt, 46.1% reported burning or stinging, 23.9% being bothered by water, 59.7% had irritation, 39% reported that their skin was sensitive and 25.4% informed of bleeding. Only 5.2% of patients never experienced itching in the 4 weeks before admission, 8.3% never experienced irritated skin and 12.3% never experienced burning or stinging. [4] Yosipovitch et al. reported that the most common associated symptoms of psoriasis were a sensation of heat in 46 patients (55%), sweating in 17 (20%) and pain in the pruritic area in 14 (17%). Patients described their itch as tickling (23%), crawling (23%) and burning (17%). The other descriptors (pinching, stinging and stabbing) were rarely reported (5%). The most common affective descriptors of itch (moderate-to-great extent) were bothersome (53%), annoying (44%), unbearable (36%) and worrisome (18%). [7] In our study we found that psoriatic patients had 96.6% pruritus, 36.8% hurting, 56.3% burning, 16.1% pain, 42.5% sensitiveness, 49.4% bleeding, 56.3% exudation, 14.9% weakness, 11.5% botheration by contact with water and 21.8% sleeplessness. Although all the other symptoms had higher frequency, only 'botheration by contact with water' symptom was less frequent in our study compared with Sampogna et al .'s study results. With a few exceptions (e.g. itching in age and education subgroups), the prevalence of symptoms in the different levels of each variable was always significantly different. [4] Sampogna et al . and Amatya et al . reported that, for all variables, the frequency of symptoms was higher in women than in men.[3],[4] Additionaly, Sampogna et al . reported in general that prevalences of symptoms were also higher in older patients than in younger ones. [4] Amatya et al . reported that occurrence of pruritus with higher pruritus intensity as well as other symptoms, such as heat sensation, pain, stinging, tickling and crawling, were more common in women than in men. [3] We also found that all symptoms were higher in females than in male and the frequency of symptoms were found to be higher in older patients, except between 41 and 50 age years of, and 'botheration by contact with water' symptom. Sampogna et al . mentioned that percentages of patients reporting that they experienced symptoms often or all the time were generally higher at lower levels of education. [4] In our study, we did not find any association between frequency of symptoms and education level of patients. Among the different clinical subtypes Sampogna et al . showed a wide variability in frequency of symptoms, e.g. pain was experienced 'often' or 'all the time' from 10.3% of patients with the guttate type to 50% of those with arthropathic psoriasis; itching from 50% in guttate psoriasis to 74.3% in the arthropathic form; bleeding ranged from 16.2% in the guttate type to 36.2% in the palmoplantar type. [4] In Szepietowski's study, presence and intensity of itching did not depend on age and gender of patients. And also the presence and intensity of itching did not depend on the clinical type of psoriasis. [8] According to the results of our study, except pruritus we found higher frequencies of exudation (50.0%) and bleeding (45.8%) in localized plaque type, burning (56.0%) in generalized plaque type, exudation (68.0%) and burning (64.0%) in guttate and other types of psoriasis. Generally, we did not observe only association between the symptoms and the clinical type of psoriasis. Another study about vulvar discomfort in female psoriasis patients revealed 41 (44.1%) women experiencing vulvar discomfort, 18 (19.4%) itching, 10 (10.8%) burning and 13 (14.0%) both itching and burning sensations. Psoriatic lesions on the vulva were found in 22 (23.7%) women. No significant correlation was found between burning or itching intensity and the global psoriasis severity ( r = 0.19, p = 0.26). Patients with vulvar discomfort had psoriatic lesions on the vulva more often than women without discomfort (43.6 vs. 8.2%, p < 0.001). In addition, patients with vulvar discomfort more frequently demonstrated depressive symptoms ( p < 0.05). They concluded that vulvar discomfort is an important clinical problem in women with psoriasis and should be taken into consideration during treatment. [9] We found that 97.8% of our female patients had pruritus, 62.2% burning, 53.3% sensitiveness, 46.7% hurting and 22.2% pain due to psoriatic lesions. Although statistically insignificant, hurting, burning, pruritus and sensitiveness were found to be in higher frequency in female patients with PASI score ≥10. In Sampogna et al .'s study, the frequency of patients experiencing symptoms 'often' or 'all the time' was generally higher at higher levels of severity, when considering both PASI and self-administered PASI scores. [4] Also, the prevalence of symptoms was significantly higher in patients with psychiatric morbidity than in those without psychiatric morbidity, for each symptom considered. They showed that symptoms had high prevalences even in patients with low or very low PASI scores (i.e. < 5). They also concluded that the exclusion of a standardized measure of symptoms was a serious limitation of PASI, and that an instrument providing a more meaningful assessment of severity of psoriasis should include a structured measurement of symptoms. [4] Szepietowski et al . found in their study that the severity of psoriasis in pruritic patients was significantly ( p < 0.004) higher as compared to nonpruritic subjects. Significant correlations were found between PASI scores and intensity of itching. [8] In another study of Szepietowski et al ., the clinical severity of psoriasis in pruritic patients [Psoriasis Area and Severity Index (PASI) score 19.1 ± 12.8] was significantly ( p < 0.004) increased in comparison with nonpruritic subjects (PASI 11.4 ± 9.4). [10] In Chang et al .'s study, of the 152 patients with psoriasis, 112 (73.7%) had pruritus, and these patients had a higher mean PASI score than psoriatic patients without pruritus. There was a positive correlation between the PASI score and the intensity of pruritus. [11] Otherwise, Amatya et al . did not find significant association between the intensity of pruritus and the extent of psoriasis. [3] Nakamura et al . did not observe a relationship between pruritus and severity of psoriasis. [12] In our study, only 'weakness' symptom was found to be significantly higher in PASI ≥ 10 patients ( p = 0.041). The frequency of other symptoms were higher (hurting, burning, pruritus, sensitiveness, sleeplessness), equal (botheration by contact with water) or less (pain, bleeding, exudation) in PASI ≥ 10 patients. It is relevant to note that PASI, the most commonly used measure of severity of psoriasis, does not take symptoms into account. This could have been based on the assumption that a perfect correlation exists between PASI scores and the presence and frequency of symptoms. Pruritus is a chronic symptom which may lead to depression and affect the quality of life in many patients. Studies have reported that not only does stress modulate pruritus, but that severe pruritus is stressful for psoriatic patients. [13],[14] Mood, concentration, sleep, sexual desire and appetite were negatively affected by pruritus. [3],[15] In our study, we also examined relationships between symptoms, quality of life scores and depression status. The frequency of whole symptoms, not only pruritus, were higher in DLQI ≥ 10 patients. Sensitiveness ( P = 0.004), weakness ( P = 0.017) and botheration by contact with water ( P = 0.008) were found to be significantly high in these patients. We also found that the prevalence of pain was statistically higher in the presence of depression as determined by the Hamilton depression scale ( P = 0.019). Also prevalences of other symptoms (except weakness) were found to be higher in depressive psoriatic patients compared with nondepressive psoriasis patients. As a result of this study, we suggest that dermatologists should be alert to the presence, frequency and relevance of symptoms experienced by their patients with psoriasis on the evaluation of disease severity both in clinical practice and in clinical trials. It is also important to interrogate these associated symptoms before deciding therapeutic approaches and evaluating their efficacies. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09188t1.jpg] [dv09188t2.jpg] |
| |||||||||

{kind=link}
{kind=link}