 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
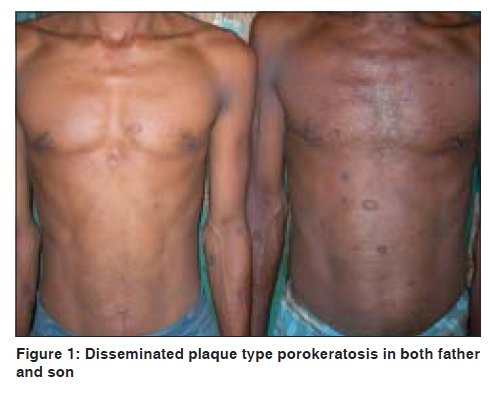
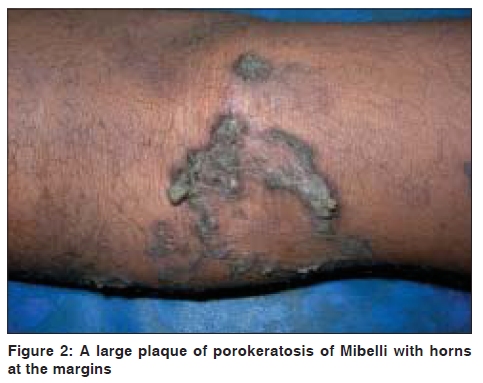
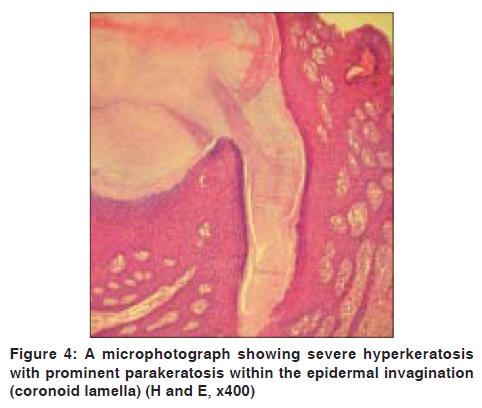
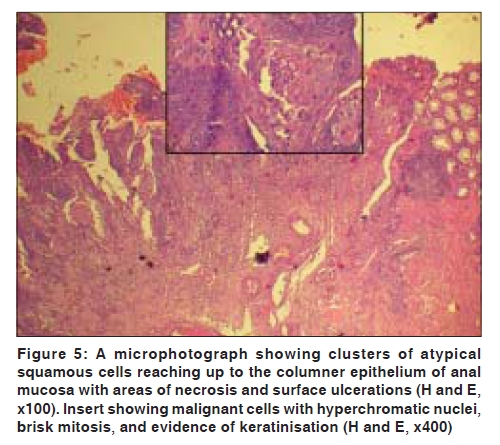
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 551 Net Case Familial disseminated plaque type porokeratosis with multiple horns and squamous cell carcinoma involving anal skin Nilendu Sarma, Anup Kumar Boler1, Sneha Ranjan Bhattacharya Departments of Dermatology, 1Pathology, NRS Medical College, Kolkata, India. Code Number: dv09189 PMID: 19736460 DOI: 10.4103/0378-6323.55427 Abstract Porokeratosis is a disorder of keratinization showing a well-defined lesion with a hyperkeratotic ridge on the border that contains the coronoid lamella. We report familial (autosomal dominant with reduced penetrance) disseminated plaque type (Mibelli's type) porokeratosis in a father and son. In the father, there were multiple horns and a large squamous cell carcinoma in a large lesion over the perianal region that reached up to the squamo-columnar junction of the anal mucosa and even invaded the anal sphincteric muscles. Disseminated lesions of the Mibelli's type, development of horns, and malignancy in this unusual location have not been previously reported.Keywords: Porokeratosis of Mibelli, Anus, Familial, Horns, Squamous cell carcinoma Introduction Porokeratosis is a rare disorder of keratinization clinically characterized by a hyperkeratotic ridge on the border and a stack of parakeratosis (coronoid lamella). Etiopathogenesis of porokeratosis is unknown but genetic inheritance as well as acquired form has been reported. Common types of porokeratosis are Mibelli's type, disseminated superficial type, (actinic and non actinic variety), linear type, etc. Distinction between these types is made purely on clinical criteria. Combination of different varieties is reported but disseminated or numerous lesions in Mibelli's type is rarely reported. [1] We report two cases of disseminated familial porokeratosis of Mibelli in a father and son. The father had multiple horns and a large squamous cell carcinoma (SCC) in a large lesion over the perianal region extending up to the squamo-columnar junction of the anal mucosa and sphincteric muscles. Case Report A 51-years-old male and his 23-year-old son presented to us with multiple, well-defined, annular oval, polycyclic or irregular shaped lesions with raised margins. All the lesions were dark brown and were widely distributed both in the exposed as well as the covered areas. They were dry, palpable, and the margins were elevated compared with the central area. Along the margin, there was a prominent deep furrow [Figure - 1]. Most of the lesions measured 4-6 cm in their longest dimension and were slightly larger in size in the father. The father had some additional features. Many lesions, even smaller ones, showed a tendency towards development of gross hypertrophy in the margin with well formed horns in some [Figure - 2]. The central part of the lesions showed clinically normal skin in most lesions [Figure - 3]. Some lesions also appeared warty with a prominent break on the entire surface. In the father, there was a large ulcer (8 x 9 cm) over both the buttock and perianal areas with predominant lateral extensions towards the patient's left side (at 3 to 6 o' clock) and towards the patient's right side (9 to11 o' clock). The ulcer was surrounded by typical lesions with hyperkeratotic margin. The ulcer involved the anal margin exposing the mucosal layer that appeared mildly prolapsed. There were also multiple lesions scattered over the buttocks; their sizes were 3 to 6 cm and mostly oval in shape [Figure - 3]. Considering the clinical presentation, we diagnosed these cases as disseminated Mibelli's plaque type porokeratosis with multiple horns and an ulcer in the father. The father's grandmother, his both sons (including one who attended), and daughter had similar diseases. His father was asymptomatic until 33 years of age when he died of unknown cause. His mother did not have the same disease. All who had the disease started to develop the lesions during the age of 12-15 years. Histological examination of the lesion was done in the father from two sites; one from the margin of a well-defined hyperkeratotic lesion over the foot and another from the ulcer in the perianal region. Histology from the margin of clinically typical porokeratosis over the foot showed a column of severe hyperkeratosis and epidermal invagination filled with parakeratosis (coronoid lamella). The subepidermal stroma showed mild infiltration of lymphocytes [Figure - 4]. This histomorphological feature was consistent with our clinical diagnosis of porokeratosis. A histopathological examination of the ulcer in the perianal region showed atypical squamous cells in clusters and sheets with surface ulceration [Figure - 5]. The squamous cells showed moderate pleomorphism, hyperchromatic nuclei, and prominent nucleoli. Brisk mitosis and focal necrosis were observed [Figure - 5]. Keratin pearl and evidence of intracytoplasmic keratin were noted. On the basis of these histological features, a diagnosis of keratinizing squamous cell carcinoma was made. The tumor involved the anal canal reaching up to the squamo-columnar junction in its upper part. The anal sphincteric muscles were also infiltrated by the tumor. A histological examination of a skin lesion on the back from the son also showed features consistent with porokeratosis of Mibelli. Finally, the cases were confirmed as familial porokeratosis of Mibelli's type with secondary squamous cell carcinoma over the buttock involving the anus in the father. Unfortunately, the patients were lost during the work-up period even before any therapeutic intervention could be made. Discussion Heredity, immunosuppression, infection, and ultra-violet rays have been found to play a role in the causation of porokeratosis. Autosomal dominant mode of inheritance has been reported in all forms of familial porokeratosis. Linear porokeratosis is said to represent the type 2 segmental form of the disease. [2] No specific candidate gene has been found. However, genetic loci of disseminated superficial actinic porokeratosis has been detected in the region 12q23.2-24.1 (DSAP 1) and 15q25.1-26.1 (DSAP 2). Recently, another loci has been found within an 8.2 cM or 11.9 Mb region between markers D1S438 and D1S464 (DSAP 3). [3] No gene or genetic locus has been found specifically for Mibelli's type. The pattern of inheritance in the family of our cases clearly indicated an autosomal dominant mode of inheritance. There was a history of involvement in four successive generations except the second generation. Absence of manifestation in the second generation was most likely the result of the phenomenon called reduced penetrance. The plaque type variety is characterized by larger lesions, a prominent raised wall with a distinct furrow, and a limited number of lesions. This specific variety was originally described by Mibelli. [4] In contrast, in the disseminated superficial form, the lesions are many, much smaller, and have only minimally raised, less hyperkeratotic border sometimes even without a prominent furrow. The distinction between the different clinical types is dependent on the clinical appearance. A disseminated lesion of Mibelli's type is only occasionally reported. [1],[5] The concomitant presence of different clinical patterns in a single case has been found repeatedly. Among the atypical presentation, few cases of hypertrophic, verrucous, or nodular porokeratosis have been reported recently in the literature. [6] In all these cases, whole lesions appeared keratotic and nodular. However, extreme hypertrophy localized in the marginal areas resulting in the development of multiple horns as seen in the present case has not been reported. Malignancy, although rare, has been reported in almost all forms of porokeratosis. Larger lesions have higher malignant potentiality, particularly, the giant variety that is most frequently reported to show malignant transformation. Higher malignant potentiality of the giant form was evident especially when multiple patterns presented in a single patient but malignancy developed in the giant lesion. [7] In the present case, SCC developed in a large lesion. SCC is the most commonly reported malignancy in porokeratosis. Other malignancies reported in porokeratosis are Bowen's disease, basal cell carcinoma, diffuse large B-cell lymphoma, etc. Areas other than skin, such as the cornea, [8] oral, [9] and other mucosa [10] have been reported to be involved with porokeratosis. To the best of our knowledge, so far, no case of porokeratosis has been reported where SCC arising from porokeratosis involved the anal canal extending up to the squamo- columnar junction. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09189f4.jpg] [dv09189f5.jpg] [dv09189f2.jpg] [dv09189f3.jpg] [dv09189f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}