 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
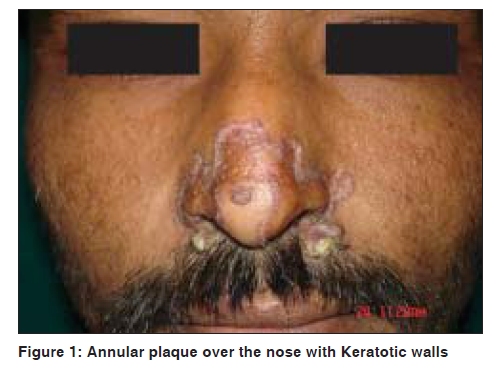
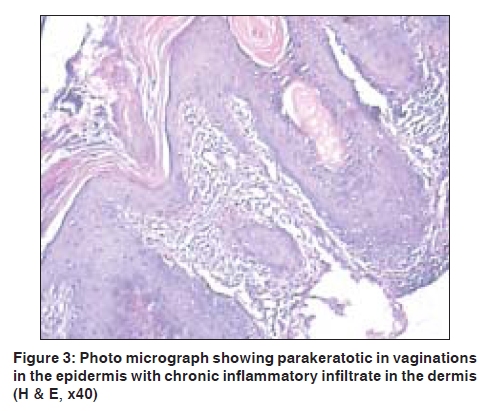
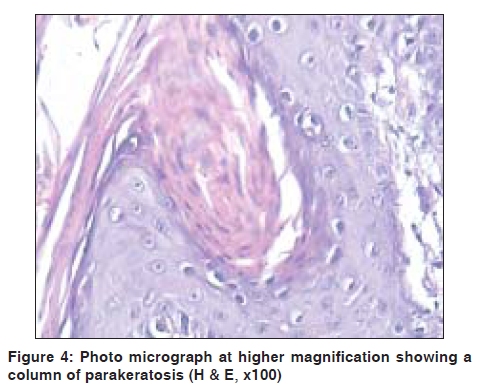
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 5, September-October, 2009, pp. 552-553 Net Quiz Large annular plaque with central atrophy on nose Raju G. Chaudhary, Freny Bilimoria, S. K. Katare Department of Dermatology, Kesar SAL Medical College and Research Institute, Ahmadabad, India Code Number: dv09193 PMID: 19736462 DOI: 10.4103/0378-6323.55432 A 21-year-old man presented with a 2-year history of an asymptomatic small, single papular lesion on the left side of the nose, which gradually increased in size with central clearing. The patient was otherwise healthy. There was no incidence of a similar disorder in his family. Examination revealed a large (>10cm) annular plaque surrounded by well-defined keratotic walls, which revealed a thin groove on close inspection, with central atrophy on the nose involving alae nasi, upper part of the lip and vestibule of the nose with wafer scales [Figure - 1] and [Figure - 2]. The findings of all routine investigations were within normal limits. Results of HIV antibody test and Mantoux test were negative. Collagen profile was within normal limits. Histological examination of the tissue from the lesion on the left side of nose showed multiple follicular and parakeratotic invaginations in the epidermis, absent granular layer and scattered dyskeratotic cells. Underlying dermis showed chronic inflammatory infiltrate [Figure - 3] and [Figure - 4]. What Is Your Diagnosis?
Discussion Porokeratosis of Mibelli is a rare genodermatosis of abnormal epidermal keratinization. Clinically, it is characterized by annular plaques with a raised horny border that spreads centrifugally with a histological hallmark of cornoid lamella. [1],[2] It may be inherited as an autosomal dominant trait with incomplete penetrance or may result from somatic mutation. Triggering factors such as irradiation, trauma, and immunosuppression may affect abnormal clones of cells that may result in abnormal keratinization. [3] Porokeratosis of Mibelli, first described by Mibelli in 1893, occurs at any age and is more common in childhood. In non-hereditary cases, however, lesions may appear at a later stage. It is two to three times more common in men than in women. According to Schamroth et al ., porokeratosis (PK) types can be divided clinically into localized form of porokeratosis of Mibelli including classic (CPK or plaque type), linear, punctuate and disseminated form including disseminated superficial porokeratosis (DSPK), disseminated superficial actinic porokeratosis (DSAPK) and PK palmaris plantaris et disseminata. [4] Apart from the above mentioned variants, a number of morphological forms such as facial PK, giant PK, punched out and reticulate PK have been reported. Giant classical PK and linear form of PK are more prone to develop of malignant changes. General measures such as lubrication and use of keratolytics may improve symptoms when present. Small circumscribed lesions can be removed by surgical cryotherapy, excision or laser therapy. Isolated studies have reported various responses to treatment with topical or intralesional cortisone, topical hydrocortisone, topical 5FU, topical tretinoin and systemic etretinate. A classical form of PK on the nose is rare to be seen and it is easily confused with other chronic disorders of skin such as annular discoid lupus erythematosus (DLE), sarcoidosis and lupus vulgaris. Here, we report a 21-year-old man who showed the giant variant of classical plaque PK. Porokeratosis is today recognized as a keratinization disorder, with a familial and premalignant tendency. The development of malignant lesions such as squamous cell carcinoma, Bowen's disease and basal cell carcinoma in PK of Mibelli has been observed on some occasions. Sasson and Krain and several other studies have shown that elderly patients and those with the long-standing disease are at the greatest risk of neoplastic transformation. The linear (LPK) and classic PK types seem to have the highest malignancy rate, whereas SADP, PPPD and PKP have lower risk rates. Sasson and Krain concluded in their review that linear or coalescent lesions contain many mitotic cells and the epidermis is hypertrophic, thus more susceptible to malignant transformation. [5] Porokeratosis of Mibelli is considered to be an uncommon skin problem. Patients seldom seek medical care because lesions may remain asymptomatic. Actually, patients seem to seek specialized medical advice only when lesions become esthetically unacceptable. Patients with porokeratosis of Mibelli should periodically undergo dermatological examination and early neoplastic lesions should be submitted for biopsy. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09193f4.jpg] [dv09193f1.jpg] [dv09193f2.jpg] [dv09193f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}