 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
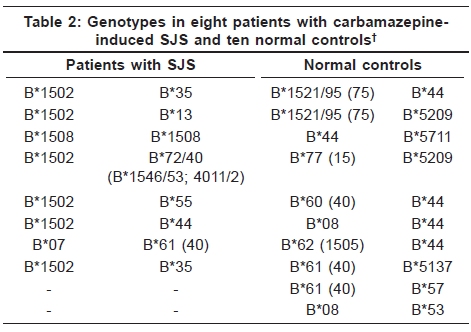
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 579-582 Original Article Association of HLA-B*1502 allele and carbamazepine-induced Stevens-Johnson syndrome among Indians Timir Y. Mehta, Laxman M. Prajapati1, Bharti Mittal2, Chaitanya G. Joshi3, Jayesh J. Sheth4, Dinesh B. Patel5, Dinkar M. Dave, Ramesh K. Goyal6 Dr. Rasiklal Shah Sarvajanik Hospital, Modasa 383315, Code Number: dv09199 PMID: 19915237 DOI: 10.4103/0378-6323.57718 Abstract Background: Stevens-Johnson Syndrome (SJS) and toxic epidermal necrolysis are severe cutaneous reactions caused by certain drugs, including antiepileptic carbamazepine. A strong association has been reported between human leucocyte antigen (HLA)-B*1502 and carbamazepine-induced SJS in Han Chinese patients. European studies suggested that HLA-B*1502 is not a universal marker but is ethnicity-specific for Asians.Aim: To study the association between HLA-B*1502 and carbamazepine-induced SJS in Indian patients. Methods: Eight individuals who fulfilled the diagnostic criteria of SJS induced by carbamazepine were identified and HLA-B molecular typing was performed. HLA-B genotyping was carried out by polymerase chain reaction using sequence-specific primers. Results: Out of eight patients studied for genotype, six patients were found to have the HLA-B*1502 allele. Conclusion: This study suggests an association between HLA-B*1502 and carbamazepine-induced SJS in Indian patients. Keywords: Carbamazepine, HLA-BFNx011502, Hindu, Indian, Stevens-Johnson syndrome Introduction Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are acute life-threatening reactions of the skin to drugs. SJS and TEN are two related mucocutaneous blistering disorders with significant mortality (especially with TEN) and prolonged morbidity. Patients develop an acute exanthema, which progresses toward a widespread blistering (TEN) or more limited purpura, vesicles (SJS) and erosion of the skin and mucous membranes, resulting from apoptosis of keratinocytes. The incidence of SJS is estimated to be one to six cases per million person-years and of TEN at 0.4-1.2 cases per million person-years. Various drugs are reported to be associated with a high risk for SJS and TEN. These include several antiepileptic agents, especially carbamazepine, phenytoin, phenobarbital and lamotrigine, antibacterials, anti-inflammatory drugs of the oxicam family and allopurinol. [1],[2] Chung and colleagues [3] reported a very strong association between carbamazepine-induced SJS in Han Chinese patients and the human leucocyte antigen (HLA)-BFNx011502 allele. They studied 44 Han Chinese patients with carbamazepine-induced SJS and two groups of controls, 101 tolerant patients and 93 healthy controls. All 44 SJS or TEN patients had an HLA-BFNx011502 allele in contrast with 3% of the carbamazepine-tolerant patients and 8.6% of the unexposed controls, respectively. [3] In Europe, HLA-B genotyping was carried out in 12 patients of carbamazepine-induced SJS. Of the 12, only four had HLA-BFNx011502. Remarkably, all the four had an Asian ancestry and originated from China, Vietnam, Cambodia, and the Reunion Island. It was suggested that HLA-BFNx011502 is not a universal marker for carbamazepine-induced SJS but is ethnicity-specific for Asians. [4] Studies in other Asian populations from Malaysia, Thailand and Hong Kong have also reported an association between HLA-BFNx011502 and SJS induced by carbamazepine. [5],[6],[7] None of these studies have been reported from India although the incidences of SJS were found to be higher among Indians compared with Europeans. [8],[9],[10],[11] Carbamazepine is a widely prescribed antiepileptic in India and is found to be the most commonly implicated drug responsible for SJS/TEN among Indians. [12] In the light of the above observations, we have undertaken an HLA genotyping study of Indian patients suffering from carbamazepine-induced SJS. Methods Patient recruitment and sample collection Eight individuals who fulfilled the diagnostic criteria of SJS induced by carbamazepine were identified at Dr. Rasiklal Shah Sarvajanik Hospital and Samarpan Centre for Treatment of Diseases of Skin, STD and Leprosy, Modasa, India. All the patients were assessed by dermatologists who had received photographs, pathological slides and medical records. Patients with definite diagnosis and ready to sign written consent were included in the study. Ten unrelated normal controls from the same population were selected randomly. The study was approved by the Institutional Review Board of Dr. Rasiklal Shah Sarvajanik Hospital, Modasa. The diagnostic criteria of SJS were based on the clinical morphology defined by Roujeau. [13] We defined SJS as skin detachment up to 10% of the body surface area and overlap SJS/TEN as skin detachment of 10-30%. Our five patients (no. 2, 3, 4, 7, 8) received carbamazepine as an antiepileptic therapy. Two patients (no. 5, 6) received carbamazepine as a post head injury anticonvulsant prophylaxis. In the remaining one patient (no. 1), trigeminal neuralgia was the indication for carbamazepine. Peripheral blood was collected in ethylene diammine tetra acetic acid-coated sterile vials and stored in a refrigerator. [Table - 1] shows the clinical characteristics of eight patients with carbamazepine-induced SJS identified in our study. DNA extraction Genomic DNA from peripheral lymphocytes was extracted by the standard phenol-chloroform method. HLA-B genotyping The quality and quantity of the extracted DNA was checked on 0.8% agarose gel and a spectrophotometer. The concentration of each DNA sample was finally adjusted to 30 ng/µl, which was used for HLA-B molecular typing. HLA-B genotyping was carried out by polymerase chain reaction (PCR) using sequence-specific primers (Micro SSP HLA-B kits; One Lambda Inc., Canoga Park, CA, United States. Low-resolution HLA-B genotyping was carried out with the One Lambda HLA-B kit in a PCR with sequence-specific primers according to the protocol and recommendations of the manufacturer (PCR-SSP, One Lambda Inc.). Statistical analysis Allele frequency between the two groups was compared by the Chi-square method with Yates' correction by constructing 2 x 2 tables. The odds ratio was calculated with Haldane's modification, which adds 0.5 to all cells to accommodate a possible zero count. Results We determined the HLA-B genotypes of eight carbamazepine-induced cases and 10 normal controls by PCR using sequence-specific primers (Micro SSP HLA-B kits; One Lambda Inc.). We found that six out of eight patients had the HLA-BFNx011502 allele (all being heterozygous). One patient was found to be homozygous with HLA-BFNx011508 allele. All the 10 controls were found to be negative for HLA-BFNx011502. The genotypes observed are shown in [Table - 2]. The odds ratio was found to be 71.40 (95% CI, 3.0-1698) and the P-value was found to be 0.0014. Discussion HLA-BFNx011502 as a marker for carbamazepine-induced SJS is well established in the Han Chinese by different studies. The allele frequency of HLA-BFNx011502 in the Han Chinese population is 8%, which is relatively higher than any other population of the world. [14] From India, a 0-6% (average 2.5%) prevalence of HLA-BFNx011502 in different communities has been reported. Most of them are sub-Hindu communities, except Parsi, in which a 0% prevalence is reported. [15],[16],[17],[18],[19],[20] Our eight patients also belong to the Hindu community, which is the biggest community of India comprising of one billion Indians. Our six out of eight patients had HLA-BFNx011502 while none of the 10 controls were found to be positive. This clearly indicates a significant association (Odds ratio: 71.40 [95% CI, 3.0-1698]; P = 0.0014) between carbamazepine-induced SJS and HLA-BFNx011502 among Indians. Because the association is not 100%, as observed in the Han Chinese community, other genes or combinations of genes might be playing a role. To conclude, we suggest HLA-BFNx011502 testing before initiating carbamazepine drug therapy in Indians. To obtain a clear Indian picture, the study should be extended to different subethnic groups from different regions. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09199t1.jpg] [dv09199t2.jpg] |
| |||||||||


{kind=link}
{kind=link}