 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 596-599 Case Report Cutaneous zygomycosis: A possible postoperative complication in immunocompetent individuals Ragini Tilak, Prabhat Raina1, Sanjeev Kumar Gupta1, Vijai Tilak2, Pradyot Prakash, Anil Kumar Gulati Departments of Microbiology,
1General Surgery, 2Pathology,
Institute of Medical Sciences,
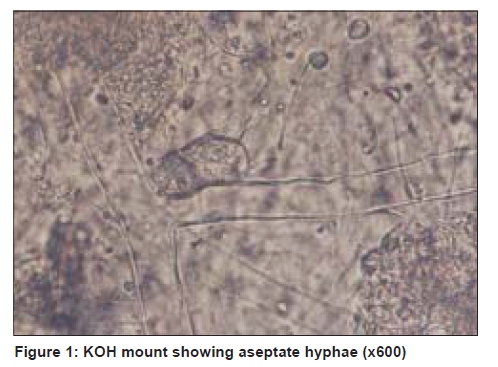
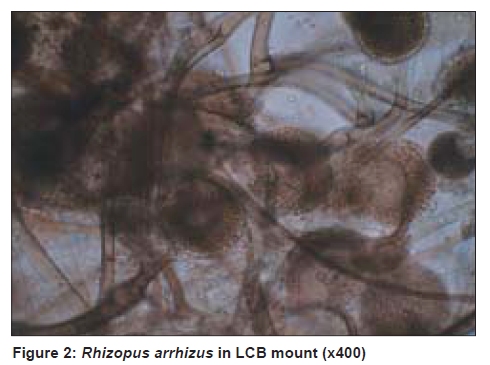
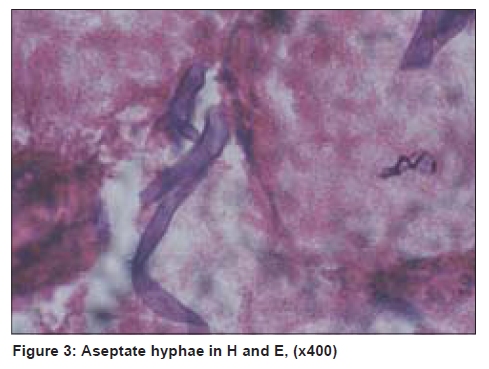
BHU, Varanasi, India Code Number: dv09203 PMID: 19915241 DOI: 10.4103/0378-6323.57722 Abstract Fungi in the class of zygomycetes usually produce serious infections in diabetics and immunocompromised hosts. Cutaneous zygomycosis is a less common form, with an unpredictable extent of anatomical involvement and clinical course. Here, we report two cases of primary cutaneous zygomycosis as postoperative complications in otherwise healthy females. Zygomycosis was suspected and specimens from the surgical debridement were examined by microbiological and histopathological studies for confirming the clinical diagnosis. Rapid diagnosis, liposomal amphotericin B, and proper debridement of affected tissue are necessary to avoid a fatal outcome.Keywords: Potassium hydroxide preparation, Cutaneous zygomycosis, Immunocompetent host, Rhizopus arrhizus Introduction Zygomycosis is caused by saprophytic fungi belonging to the class Zygomycetes and the order Mucorales. On the basis of clinical presentation and site of infection, mucormycosis can be divided into six clinical categories: (i) rhinocerebral, (ii) pulmonary, (iii) cutaneous, (iv) gastrointestinal, (v) disseminated, and (vi) miscellaneous. [1] Primary cutaneous zygomycosis, which accounts for about 16% of the cases, may prove fatal if treatment is delayed. [2] Here we report two cases of cutaneous zygomycosis of the anterior abdominal wall, as a postoperative complication, in otherwise healthy young females. Case Reports Case 1 A 26-year-old female underwent ovarian cystectomy through a lower midline laparotomy for a twisted ovarian cyst. On the eighth postoperative day, she developed cellulitis around the incision site. She was started on empirical treatment with routine conventional antibacterial therapy, namely, ceftriaxone 2 gm intravenous (iv) bd, amikacin 500 mg iv od, and metronidazole iv, thrice daily. Subsequently, she developed necrosis of the surrounding abdominal wall, which did not improve despite debridement. She was having high-grade fever and the wound continued to progress peripherally. She was then referred to the University Hospital, Banaras Hindu University, Varanasi. At the time of presentation, she was ill and was complaining of pain. Her temperature was 39°C, heart rate was 108 beats / minute, respiratory rate was 22 breaths / minute, and blood pressure was 160 / 80 mm of Hg. An abdominal examination revealed a large area of about 15 cm × 12 cm of skin and subcutaneous tissue loss in the lower abdomen with pale granulation tissue at the base. Edges were erythematous, firm, indurated, and rolled inwards. There was no history of diabetes, malignancy, or any other evidence of an immunocompromised status. Her total leucocyte count was 18,000 / mm 3 with 87% neutrophils. Other blood parameters were within normal limits. A diagnosis of postoperative synergistic gangrene of the anterior abdominal wall was made. Aerobic and anerobic cultures for bacterial infection were negative. Two blood specimens were also collected for fungal and bacteriological culture; however, both were found to be sterile. Despite seven days of antibiotic therapy, repeated debridement, and daily dressing, fever persisted and total leucocyte count increased to 30,000/mm3. The wound did not show any sign of improvement. The area of erythema, induration, and necrosis continued to grow peripherally. Later a white cotton wool-like material was identified on the margins of the wound. Wound tissue was sent for potassium hydroxide (KOH) mount, fungal culture, and histopathologic examination. Microscopic examination of the KOH mount of the wound tissue showed broad nonseptate hyphae [Figure - 1] and amphotericin B was started immediately. Culture of the necrosed tissue on Sabouraud's dextrose agar showed filamentous fungus, which was provisionally identified as a Rhizopus species [Figure - 2]. Colonies of Rhizopus grew rapidly, filled the petri dish in two days, and matured in four days. The texture was typically cotton candy like. From the front, the color of the colony was white initially and turned gray to yellowish brown in time. The reverse was white to pale. The lactophenol cotton blue preparation showed mycelia, which were wide, aseptate, with rhizoids coming off directly from the stolon and sporangiophore. The sporangia were round and filled with spores. The sporangiospores were unicellular, round to ovoid in shape, hyaline to brown in color, and striated in texture. [3] The mold was finally identified as Rhizopus arrhizus. A histopathologic examination revealed aseptate hyphae that appeared to divide at varying angles up to right angles, with perivascular polymorphic infiltration [Figure - 3]. After six days of amphotericin B treatment, the fever subsided and the wound base started granulating. Total leucocyte count decreased to 8000/mm 3 . She started feeling well. On the eighth day of antifungal treatment she suddenly developed dyspnea and collapsed. Despite resuscitative measures she could not be revived and she expired on the twenty-eighth postoperative day. Case 2 A 24-year-old female delivered a male child by cesarean section. A midline incision was given in the lower abdomen for cesarean section. The patient was on broad spectrum antibiotic prophylaxis. On the fourth postoperative day, she developed cellulitis on the right side of the incision site. none The patient received empirical antibiotic therapy, including ceftriaxone 2 gm iv bd, amikacin 500 mg iv od, and clindamycin 600 mg orally, thrice daily. Antibiotics were administered subsequently, but she developed necrosis of the surrounding abdominal wall, which did not improve despite debridement. She was referred to the University hospital, BHU. At the time of presentation, she was febrile. Her temperature was 39.4 o C. She had pallor and increased heart rate. Her blood sugar, blood urea, and serum electrolytes were found to be normal. However, there was polymorphonuclear leucocytosis, wherein, the total leucocyte count was 16000/mm 3 with 85% neutrophils. The wound was about 12 x 8 cm in size. Wound swab and blood were sent for bacterial culture. These were reported as sterile. Despite antibiotic therapy, the fever persisted. Repeat swabs and debrided wound tissue were taken and send to the mycological laboratory. KOH mount showed broad aseptate hyphae, suggestive of zygomycosis, and a fungal culture was done on Sabouraud's dextrose agar with and without cycloheximide and incubated at 25 o C and 37 o C. A rapid, white fluffy growth was observed after 48 hours on none Sabouraud's dextrose agar without cycloheximide, which became gray in color on continued incubation and was provisionally identified as Rhizopus species. This mold was identified as Rhizopus arrhizus. A histopathologic examination revealed aseptate hyphae that appeared to divide at varying angles up to right angles, with perivascular polymorphic infiltration. Based on the above findings, a diagnosis of cutaneous zygomycosis was made. Local debridement was carried out and liposomal amphotericin B administered at a dosage of 4 mg/kg/day intravenously over 14 days. Discussion Among the member species of Zygomycetes, Rhizopus arrhizus (Rhizopus oryzae) is by far the most common cause of Zygomycosis. [3] These are widespread in nature, subsisting on decaying vegetation and diverse organic materials. The most common route of transmission is inhalation of spores from the environment. For this reason rhinocerebral and pulmonary zygomycosis are the usual types of infections in immunocompromised patients, followed by gastrointestinal, cutaneous, and disseminated infection. Primary zygomycosis of the skin and wounds has been associated with burns, traumatic disruption of skin, persistent maceration of skin, and use of contaminated elasticized surgical bandages. [4],[5] Cutaneous zygomycosis has also been reported following insect bite and tattooing. [6] Cutaneous mucormycosis can be invasive locally and can penetrate from the cutaneous and subcutaneous tissues into the adjacent fat, muscle, fascia, and even bone. Secondary vascular invasion may lead to hematogenously disseminated infection of the deep organs. [7] Most cases have been reported to occur in immunocompromised subjects. Invasive zygomycosis tends to be associated with metabolic acidosis, hyperglycemia, corticosteroid therapy, immunosuppressive therapy for organ transplantation, neutropenia and desferrioxamine therapy. [3] Roden et al., reviewed 929 cases of zygomycosis, wherein, cutaneous zygomycosis was found to be the third most common form (19%), after sinus (39%) and pulmonary zygomycosis (24%). [7] In the present study, both patients were nondiabetic and without any evidence of other immunosuppressive illness. The possible cause of abdominal wall zygomycosis is either administration of multiple antimicrobials for a long time, or the dressing material used in the peripheral hospitals. It is also possible that there was a fungal contamination of instruments due to poor sterilization techniques in peripheral hospitals leading to local wound infection, which went undetected initially. In the first case, the initial clinical feature of which resembled Meleny's gangrene, a diagnosis was made on the basis of KOH mount, histopathologic examination, and culture isolation. However, despite starting amphotericin, which gave symptomatic relief along with improvement in laboratory parameters, the patient succumbed to her illness, probably due to pulmonary embolism. The autopsy was not performed as it was denied by the family. In the second case, liposomal amphotericin B was started immediately after direct microscopy. She responded to the antifungal drug and was discharged. Parenteral Amphotericin B coupled with extensive surgical debridement and rapid control of the underlying medical disorder can improve survival rate. Liposomal amphotericin B has fewer side effects, better tolerability, and is the treatment of choice, but its high cost is a major obstacle to its widespread use. [8] Posaconazole, an oral azole antifungal with broad activity against a variety of yeasts and molds, including zygomycetes, has emerged as a safe and efficacious therapeutic alternative. Posaconazole was recently approved for antifungal prophylaxis for high-risk patient population. [9],[10],[11] Cutaneous zygomycosis in immunocompetent individuals is less common and could easily be prevented with proper preoperative preparation and postoperative dressing of the surgical site, even in peripheral health centers, by observing a strict adherence to sterilization protocols. The conventional antibiotics used empirically for prophylaxis do not provide any antifungal coverage, hence, it is absolutely important to take adequate pre-, intra-, and postoperative precautions to prevent fungal infections. The isolated cutaneous form has a favorable prognosis, with low mortality if diagnosed and treated promptly. For the treatment to be effective it should be started early and therefore the importance of high index of suspicion followed by microbiological and / or histopathological confirmation of the clinical diagnosis is very essential. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09203f2.jpg] [dv09203f1.jpg] [dv09203f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}